▎WuXi Adapt Content Team Editor
Cardiovascular and cerebrovascular diseases are one of the most important causes of death globally, seriously threatening human health.
Whether it’s an ischemic stroke due to stenosis of an intracranial artery (or carotid artery), or coronary heart disease due to a narrowing of the coronary arteries of the heart, doctors may recommend a stent Implantation (ie, placing a stent).
So what exactly is a bracket? How does the stent fit into the blood vessel? Will there be any discomfort when placing the stent? Today, Health Press takes coronary heart disease as an example to explain it thoroughly for you.
Stent placement, also known as percutaneous coronary intervention, is an effective solution to local stenosis of the coronary lumen.
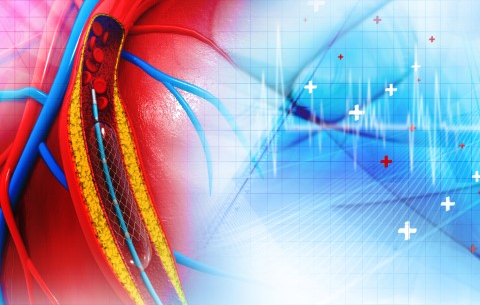
Image source: 123RF
Steps for placing the stand
First, the doctor makes a puncture in the radial or femoral artery and places a small sheath in the vessel.
This small sheath can be used for coronary angiography, allowing doctors to see where the blood vessel is blocked; it can also be used to place stents.
Then, the doctor slowly puts the stent catheter (guide wire) into the blood vessel from the sheath port, and the guide wire can be retrograde along the radial artery to the great blood vessel until the coronary port .
A guide wire is a long, thin, soft wire that acts like a train track, providing a path for the stent to be accurately delivered to the narrowed part of the blood vessel.
Inside the stent, there is a high-pressure balloon. When the stent reaches its “destination”, the doctor will open the balloon and the stent (tubular spring mesh) will be propped up.
Finally, the balloon is deflated, the balloon and guidewire are withdrawn, and the stretched stent remains in the vessel and the narrowed vessel is stretched open.

Image source: 123RF
Currently, there are bare metal stents, drug-eluting stents, and biodegradable stents. Doctors will select the appropriate stent according to the specific condition.
Classification of stents
Bare metal stent: This is the first stent to be put into clinical use, mostly made of stainless steel or cobalt-containing alloys. Compared with balloon dilation alone, it has the advantage of immediate greater lumen gain and less elastic recoil, but there is a high probability of stent restenosis (late lumen loss due to intimal hyperplasia), which is its main drawback , so only a small amount is currently used in indicated high-risk patients.
Drug-eluting stents: The first generation of drug-eluting stents, introduced in 2001, used stainless steel as a platform and a permanent polymer as a drug carrier. The rapamycin or paclitaxel inhibits the migration and proliferation of vascular smooth muscle cells locally in the blood vessel, which solves the problem of stent restenosis to a certain extent. However, the stent had an increased risk of adverse events such as thrombosis at a later stage, so it was gradually withdrawn from the historical stage.
Second-generation drug-eluting stents are mostly made of cobalt-chromium or platinum-chromium alloys, with thinner stent beams, better flexibility and delivery; antiproliferative drugs are usually liposoluble Newer zotarolimus, everolimus or other rapamycin derivatives with better biocompatibility of the polymer coating resulted in significantly lower rates of adverse events. The new generation of drug-eluting stents that are widely used at present use more advanced polymer coating technologies, including single-sided coating technology and degradable polymer coating technology.
Bioabsorbable stent: In order to avoid the permanent retention of metal foreign bodies in the body, the concept of this stent came into being. Since the first generation of absorbable stents entered large-scale clinical validation in 2006, dozens of absorbable stents around the world have entered the clinical research stage. The first product in China that uses polylactic acid as the stent matrix was officially approved by the State Drug Administration of China in February 2019, providing a new option for interventional treatment of patients with coronary heart disease.
Because there are no pain nerves in our blood vessels, the operation is performed under anesthesia, so the patient will not feel pain during the operation.

Image source: 123RF
Potential complications
Although patients who choose the transradial approach are less painful and have fewer vascular-related complications than the femoral approach, patients may be at risk for the following complications:
Acute Coronary Artery Occlusion: Patients may experience a drop in blood pressure, a slow heart rate, and even ventricular fibrillation, ventricular arrest, and more.
No-reflow: There are various ways to stabilize hemodynamics, prevent or reduce no-reflow, such as intracoronary injections of tirofiban, calcium Channel blockers, nitrates, sodium nitroprusside, adenosine and other drugs, or thrombus aspiration.
Coronary perforation: Although very dangerous, it is relatively rare.
Stent thrombosis: The incidence is 0.6% within 30 days and 2.9% within 3 years, but the mortality rate is as high as 45%. A series of measures can be used to prevent thrombosis in stents.
Finally remind everyone that although stents can improve myocardial ischemia damage, relieve chest pain symptoms, and improve heart function, it is not a one-time-for-all.
Patients need antiplatelet therapy before stenting and anticoagulation therapy during surgery. For special patients with diabetes, complex coronary artery disease, kidney disease and other diseases Antithrombotic therapy is also required.

Image source: 123RF
Postoperative rehabilitation cannot be ignored
In addition, after stenting, it is recommended that patients undergo active rehabilitation treatment, including exercise, reasonable diet, smoking cessation, psychological adjustment and drug treatment. Specifically:
Rational Diet: Control total calories and reduce intake of saturated fatty acids, trans fatty acids and cholesterol.
Weight control: Overweight and obese individuals lose 5% to 10% of their body weight within 6 to 12 months to make BMI ≤25 kg/m2; waist circumference control In males ≤90 cm, females ≤85 cm.
Quit smoking completely and avoid passive smoking.
Strictly control alcohol intake: ≤20 g/d for men and ≤10 g/d for non-pregnant women.
Pay attention to identifying the patient’s mental and psychological problems and give symptomatic treatment: such as assessing the patient’s mental and psychological state, understanding the patient’s concerns about the disease, the patient’s living environment, Friends and family relationships, and give targeted treatment measures, etc.
A study published in the Journal of the American College of Cardiology found that patients who received optimal drug therapy for 5 years after stenting or bypass surgery were All-cause mortality was lower over the next 10 years.
In addition to rational drug use under the guidance of a doctor, it is also recommended to regularly review various indicators to ensure that blood sugar, blood lipids and blood pressure are up to standard.
Also, you may also want to see:
In addition to taking medicine, how can I prevent heart disease?
What is a “normal” heart rate when exercising?
What are the top 10 risk factors for cardiovascular disease?
…

Image source: 123RF
References
[1] Interventional Cardiology Group of Cardiovascular Branch of Chinese Medical Association, Professional Committee of Thrombosis Prevention and Treatment of Cardiovascular Medicine Branch of Chinese Medical Doctor Association, Editorial Board of Chinese Journal of Cardiovascular Diseases. Guidelines for cutaneous coronary intervention (2016) [J] . Chinese Journal of Cardiovascular Diseases, 2016, 44 (5): 382-400. DOI: 10.3760/cma.j.issn.0253-3758.2016.05.006
[2] The National Center for Cardiovascular Disease (Fuwai Hospital, Chinese Academy of Medical Sciences) entrusted by the National Health Commission to lead. Coronary Balloon Angioplasty and Stent Implantation Operation Specifications (2022 Edition)
[3] Kawashima H, et al., (2021) “Impact of optimal medical therapy on 10-year mortality after coronary revascularization” J Am Coll Cardiol; DOI: 10.1016/j.jacc .2021.04.087.
Disclaimer: The WuXi AppTec content team focuses on global biomedical health research progress. This articleFor information exchange purposes only, the views expressed in this article do not represent the position of WuXi AppTec, nor do they mean that WuXi AppTec supports or opposes the views expressed in the article. This article is also not a treatment plan recommendation. For guidance on treatment options, please visit a regular hospital.
Copyright note: This article is from WuXi AppTec’s content team. Individuals are welcome to forward it to Moments, and media or institutions are not allowed to reprint it to other platforms in any form without authorization. For reprint authorization, please reply to “Reprint” on the WeChat public account of “Healthy Press Machine” to obtain instructions for reprinting.