For medical professionals only
A nearly missed perforation of the digestive tract.
The 59-year-old Aunt Zhang was recently hospitalized because of abdominal pain. In just two days, she underwent the same examination twice and stayed in the intensive care unit for a few days. How did this happen? What’s the matter?
The story happened a month ago
On February 27, 2022, Aunt Zhang was admitted to the hospital due to abdominal pain for 1 month, black stool for 4 days, and aggravation for 3 hours. After careful medical history, she found out:
The patient had abdominal pain, paroxysmal pain, no nausea, vomiting, acid regurgitation, heartburn and other discomforts without obvious incentives before 1 month, and the symptoms were slightly relieved after local oral drug treatment. No regular treatment, no gastroscopy.
4 days ago, there was no obvious incentive to expel melena once, the amount was unclear, and there was no regular examination and treatment.
3 hours ago, the patient had aggravated abdominal pain after eating raw and cold food, which was persistent, severe and unbearable, accompanied by chest tightness, palpitation, sweating, nausea, vomiting of brown stomach contents, and vomiting 3 times, the amount is about 300ml.
Therefore, immediately complete the chest, abdomen and other related examinations.
Admission physical examination: conscious, poor spirit, painful appearance, thick breath sounds in both lungs, no obvious dry and wet rales, normal heart rhythm, no heart valve auscultation area Pathological murmur, abdominal softness, whole abdominal tenderness, mainly epigastric and right lower quadrant, no rebound tenderness, normal bowel sounds, and no edema of both lower extremities.
Past history: Gynecological cyst surgery was performed 10 years ago, no postoperative discomfort; 3-year history of hypertension, oral administration of indamide tablets, nimodipine tablets and other drugs, blood pressure control is unknown ; History of type 2 diabetes for 3 months, oral metformin tablets; normal headache, intermittent oral pain medication, simvastatin tablets and flunarizine capsules and other drugs.
Auxiliary examination: admission chest + whole abdomen CT prompt (2022-02-27, our hospital): 1. Right lung cord foci; 2. A small amount of fluid in the abdominal cavity and pelvis; 3. Cystic lesions in the left adnexal area, consider cysts, and further check if necessary; 4. Double kidney stones; calcification of the left adrenal gland; 5. IUD.
Blood routine prompts: white blood cells (11.7×19/L); percentage of neutrophils (90%); neutrophils (10.56×19/L); biochemistry: glucose (28.19 mmol/L); glycosylated serum protein (4.05mmol/L); total protein (56.5g/L); globulin (18.3g/L); urea (14mmol/L); creatinine (118μmol/L); Ball filtration rate (48.2mL/min); uric acid (422.6μmol/L); sodium (129.2mmol/L); chlorine (91.3mmol/L); triglyceride (3.71mmol/L); total cholesterol (6.54mmol/L) /L).
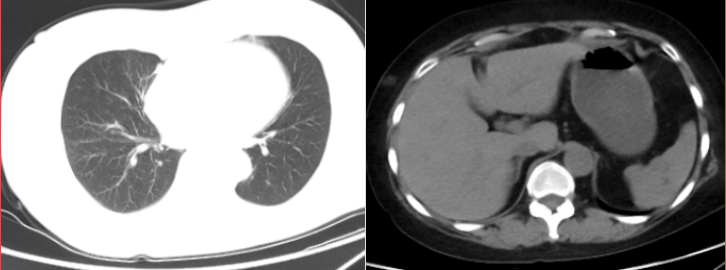
Figure 1: CT image of abdomen.
The immediate diagnosis was: abdominal pain to be investigated, type 2 diabetes mellitus, hypertension, hyponatremia.
The patient was given fasting, acid suppression, fluid replacement, laxative, enema and other treatments. The patient’s symptoms did not improve, but he still complained of shortness of breath, chest tightness, and abdominal pain.
Treatment in trouble
There is no abnormality in lung CT examination at admission. What disease can cause chest tightness, shortness of breath, and persistent abdominal pain?
There was no obvious abnormality in the CT examination at the time of admission, but the patient had shortness of breath and chest tightness. What could be the disease? ECG monitoring showed stable vital signs, slightly faster heart rate, and oxygen saturation of 98% by finger test. On admission, abdominal CT and chest CT were just done. There was no problem, but the diagnosis was still unclear. The patient’s symptoms did not relieve, but progressively worsened. , how to explain it? Severe pancreatitis? Digestive perforation? Thrombotic disease? Aortic dissection?
It appears that further tests are needed to determine the cause.
Considering the patient’s dyspnea and shortness of breath, and considering the combination of pulmonary lesions, and repeated communication with family members, it is recommended to complete the abdominal CT and chest CT examinations again.
We and our families are very entangled. What we are entangled is whether the patient has just undergone CT examination, whether there will be suspicion of repeated examination and excessive examination, and now it is stipulated that the examination results can be mutually recognized, Are we up against the wind? The patient’s family is also tangled, is it spending money? However, looking at the patient’s painful expression, I was really afraid of the patient’s accident, and finally agreed to review the CT again.
Check again, the two CT results are completely different?
As soon as the film came out, we were all shocked, but also very fortunate that if we checked it a day or two later, the consequences would be disastrous. Guess what the result is?
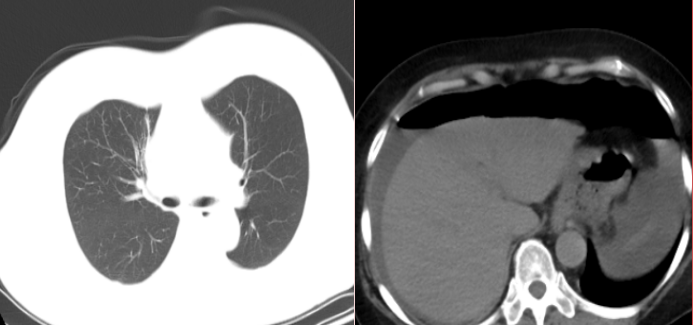
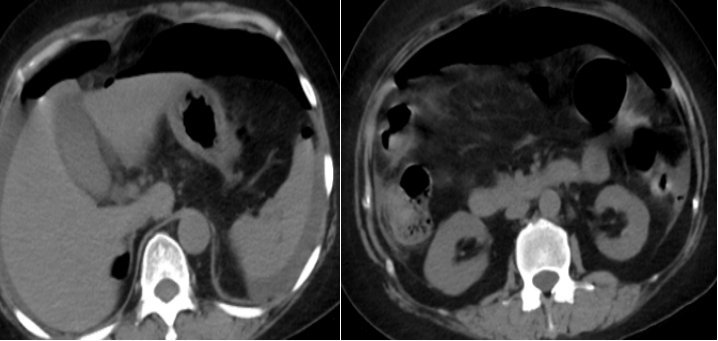
Figure 2: Abdominal CT image
It was a perforation of the digestive tract!
This is a surgical acute abdomen that requires immediate surgical treatment.
We did not dare to delay for a moment. After 7 o’clock in the evening, we immediately called the brother department. At this moment, the brother department was also very helpful. He trotted all the way over for consultation and suggested surgical treatment. The consulting doctor immediately agreed with him. The family members discussed the condition. The family members also knew the seriousness of the condition at this time and agreed to transfer the patient. We hurriedly sent the patient to the Gastrointestinal Hepatobiliary Surgery Department. The staff of the brother department worked overtime overnight to arrange the operation.
Laparoscopic minimally invasive surgery. seen during surgery. A 2x2cm ulcer was perforated in the anterior wall of the gastric antrum, the gastric wall mucosa was everted, food residues were seen around, and the ulcer was slightly hard.
After communicating with the family members, it was decided to perform laparoscopic gastric perforation suture. The operation went well and was transferred to the intensive care unit and the general ward. The patient has been discharged from hospital.
Let’s take a brief look at upper gastrointestinal perforation
Upper gastrointestinal perforation is a common clinical acute abdomen, mostly caused by upper gastrointestinal ulcers. If the perforation of the upper gastrointestinal tract is not treated timely and rationally, it will often lead to severe peritonitis or even abdominal abscess, resulting in toxemia or bacteremia, which will endanger the patient’s life.
With the accumulation of clinical experience and the continuous improvement of auxiliary examination methods, the diagnosis of upper gastrointestinal perforation is generally not difficult, and appropriate treatment methods should be selected as appropriate. If the intra-abdominal infection is not severe, there is not much perforation and exudation, or the conditions do not permit, conservative treatment can be tried. However, active surgical treatment after timely diagnosis is still the best choice for upper gastrointestinal perforation.
Lessons Learned:
1. The examination can be trusted, but not completely. The condition is developing and changing at any time, so some examinations should be done in time. CT, patients may develop septic shock, sepsis, and even death in severe cases.
2. We all know that peptic ulcers can cause bleeding and perforation. Now, with the advancement of drugs, most ulcers can be cured, and perforation of ulcers is rarely seen clinically. When encountering diabetes, multiple eyes are needed, and the patient’s abdominal toughness signs are not obvious.
3. It is recommended to check the body regularly. Those over 40 years old must have a gastroenteroscopy examination.
4. Although it is now stipulated that the results can be mutually recognized, the condition is developing and changing at any time. Some test results can be believed, and some are changed with the change of the condition. One size fits all is not suitable. Clinical work must be determined according to the condition.
The digestive case you want
Doctor’s Station “Digestive Cases” column has