For medical professionals only
Promote a multidisciplinary collaborative model to benefit patients with gastroesophageal reflux disease
Gastroesophageal reflux is one of the diseases with the highest misdiagnosis rate in clinical practice due to the diverse clinical symptoms. Academician Wang Zhonghao was once diagnosed as “bronchial asthma” because of his asthma symptoms, but he did not improve after a long period of treatment. He thought he had an “incurable disease”. It was not until later that he found out that it was gastroesophageal reflux and he was properly treated.
Which departments might gastroesophageal reflux be “lurking”? The Rocket Army Special Medical Center will take stock of 8 departments that are often involved in gastroesophageal reflux disease today. Let’s take a look.
Gastroenterology
Heartburn and reflux are the most common symptoms of gastroesophageal reflux disease, the former affecting 70%-90% of patients and the latter affecting 60%-80% of patients.
Heartburn: A burning sensation behind the sternum, however, in a small number of patients, the burning sensation may be localized or extended to the upper abdomen, retroxiphoid, anterior neck, and throat.
Reflux (acid reflux): The backflow of stomach contents through the esophagus into the mouth or pharynx without nausea, retching, and exertion, usually accompanied by Heartburn, sour or bitter taste. When it is perceived as an acidic substance, it is acid reflux, when it is food, it is antifeeding, and a few are bile or mucus.
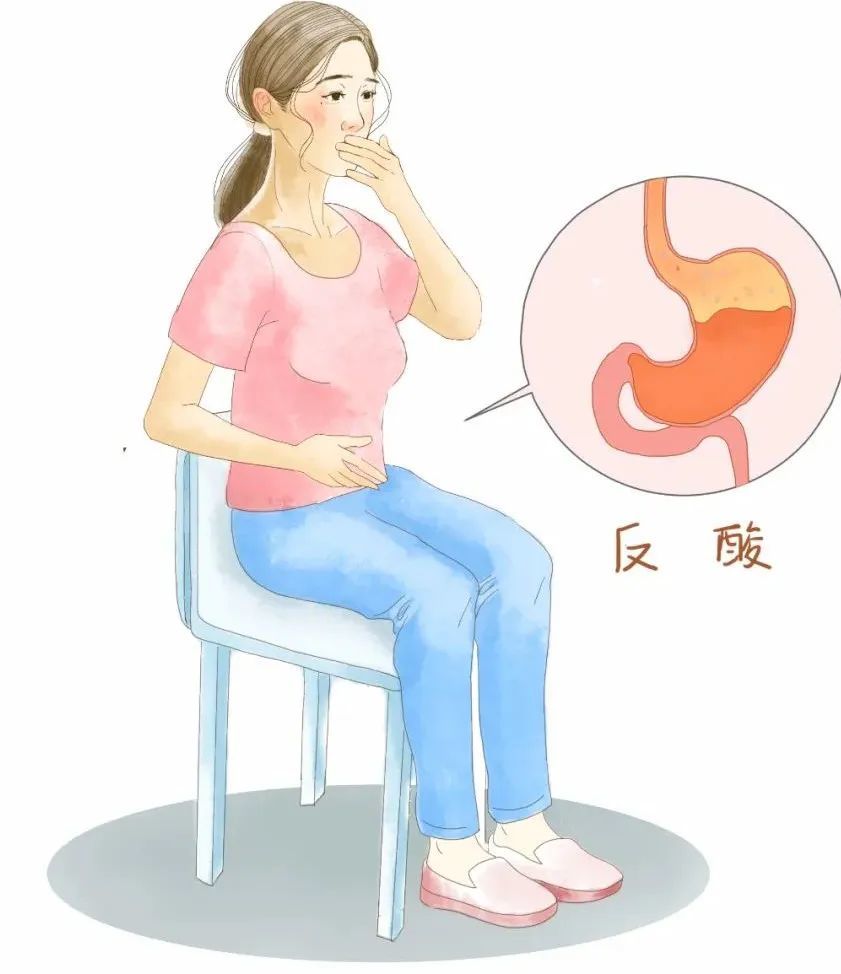
Frequent heartburn and acid regurgitation often lead to eating disturbances, sleep disturbances, life and work limitations, and poor quality of life.
Pulmonary
Gastroesophageal reflux disease is one of the most important and hidden causes of asthma. 24-hour esophageal pH monitoring in asthmatic patients showed that 53% of asthmatic patients had pathological acid reflux, and 45%-89% of asthmatic patients may have gastroesophageal reflux >. Even in asthmatics without reflux symptoms, 25% of patients with esophageal pH were found to have pathological acid reflux.
The mechanism of gastroesophageal reflux disease causing asthma is: After the gastric contents reflux into the throat, it can directly stimulate the bronchoconstriction through aerosol spray, resulting in asthma, gastric Reflux of contents into the esophagus can also cause asthma by activating the reflex arc of the vagus nerve.

ENT
High reflux of gastric contents to the throat can irritate the throat mucosa, causing congestion, edema, and lymphoid follicle hyperplasia, resulting in reflux pharyngitis. Reflux pharyngitis is a kind of chronic refractory pharyngitis, which is mainly manifested by sore throat, pharyngeal foreign body sensation, pharyngeal blockage, pharyngeal itching, cough and expectoration.
Surveys show that 4%-10% of ENT outpatients are related to gastroesophageal reflux disease. Among patients with persistent chronic pharyngitis, gastroesophageal reflux disease is as high as 34.6%.
Studies have found that reflux can not only cause dysplasia of the mucous membrane of the throat may also lead to cancer, and gastroesophageal reflux disease can increase the incidence of laryngeal, tonsil, and Risk of some sinus cancers. And with the prolongation of acid exposure, the associated risk also increases, especially laryngeal cancer and paranasal sinus cancer.
Cardiovascular
The reason why gastroesophageal reflux disease manifests symptoms of cardiovascular disease such as high blood pressure is actually because of neurological disorders. Because the innervation of the esophagus and the heart are the same, when the chemical, pharmacological or thermoreceptors of the esophageal mucosa are stimulated, it can cause chest pain similar to angina pectoris, which is easily misdiagnosed.
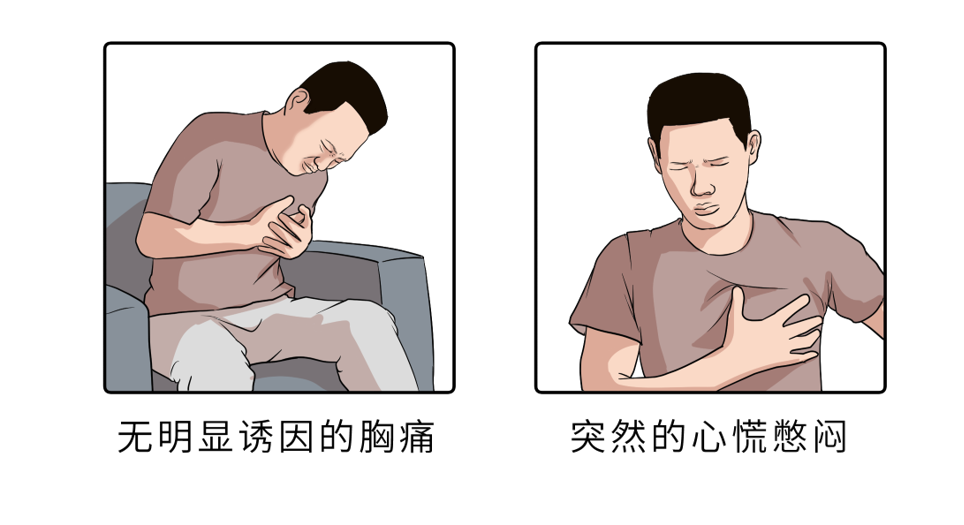
▌The pathogenesis of esophageal chest pain is:
The patient’s refluxed gastric juice and food will cause esophageal spasm, which will stimulate the nerves in the esophagus. The nerves in the esophagus will reflect the stimulation to the sympathetic and coronary nerves, causing spasm of the cardiovascular and cerebrovascular vessels. , produce angina and hypertension symptoms.
▌Esophageal chest pain is characterized by:
①The pain site is mostly located behind the sternum, under the xiphoid process or in the two rib areas, and can spread to the back, neck, jaw, upper chest, left shoulder and left arm;
②Mostly cauterized;
③ Occurs more than 1 hour after a meal, and can be induced or aggravated by lying down, bending over, squatting, coughing, and having a full meal;
④There are many nausea symptoms, such as acid reflux, nausea, etc.;
⑤There is often a feeling of food stagnation in the lower sternum after eating, accompanied by upper gastrointestinal bleeding;
⑥Due to the stimulation of the vagus nerve by chest pain, the coronary artery blood supply may be reflexively caused, and the electrocardiogram may have S-T segment changes.
Sleep Medicine and Neurology
Delayed gastric emptying, slowed esophageal motility, decreased swallowing and salivation, and prolonged clearance of esophageal contents during sleep.
Studies have shown that GERD is closely associated with a number of sleep disorders, such as decreased sleep duration, difficulty falling asleep, awakenings during sleep, and poor sleep quality , wake up early in the morning, etc. If patients with gastroesophageal reflux disease have sleep disorders, they need to be combined with sleep medicine.

Psychology
People with gastroesophageal reflux disease often also have some degree of anxiety, depression, or somatization. At the same time, frequent episodes of gastroesophageal reflux disease symptoms will affect the patient’s diet, sleep, work, social interaction, and psychology, further reducing the patient’s quality of life and social ability, and increasing the patient’s psychological burden.

The patient’s psychological factors can affect the pressure of the lower esophageal sphincter and gastroesophageal motility by regulating the level of the nervous system and gastrointestinal hormones, resulting in a significant decrease in gastric motility and delayed emptying. Increase the occurrence of gastroesophageal reflux symptoms; psychological states such as anxiety and depression can also enhance the patient’s susceptibility to gastroesophageal reflux disease symptoms, further reducing the quality of life of patients and forming a vicious circle.
The treatment of gastroesophageal reflux disease is not only to control pathological acid reflux and heal esophagitis, but also to fully relieve symptoms, improve quality of life, and stay away from anxiety and depression.
Dental
Oral and maxillofacial manifestations of GERD include tooth erosion, dry mouth, mucositis, aphthous ulcers, mouth sourness, mouth burning, hyperesthesia, bruxism, and/or Temporomandibular joint disorders, etc. The effects of chronic oral exposure to gastric contents, especially gastric acid, are diverse, causing soft tissue symptoms (nonspecific burning and sensitivity) and pathological soft tissue damage.

Surgery
In the past, the treatment of gastroesophageal reflux was mainly to suppress gastric acid by taking drugs, but the main purpose of drug treatment is to reduce the acidity, esophageal motility, hiatal hernia and other structures There is no fundamental cure for sexual deficiencies. However, the traditional surgical operation has a good therapeutic effect due to its large incision and excessive adverse reactions, but the postoperative recovery of patients is poor.
With the introduction and development of endoscopic treatment and laparoscopic surgery, the techniques of endoscopic and laparoscopic treatment of gastroesophageal reflux disease have been gradually improved. Surgery has the advantages of less trauma, better recovery and better cosmetic results, minimally invasive surgery has now become the first choice for surgeons in the treatment of gastroesophageal reflux disease.
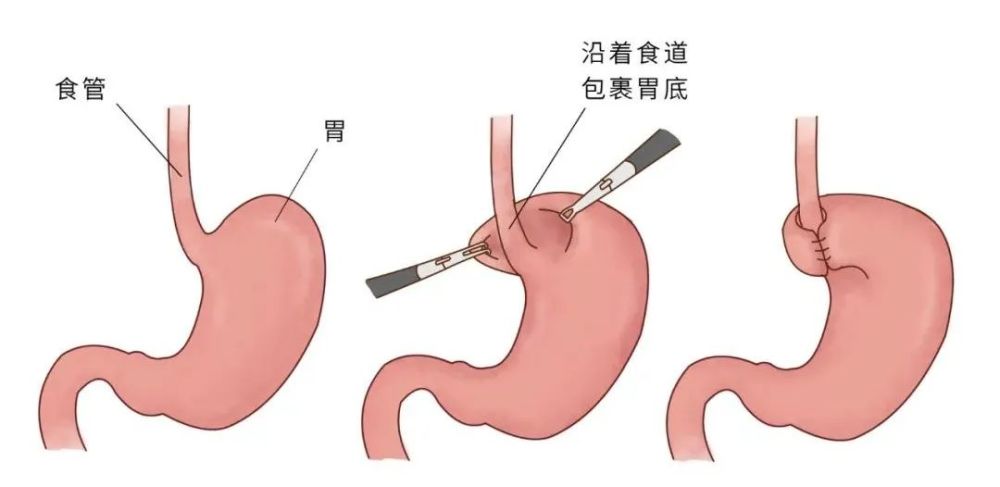
Gastroesophageal reflux minimally invasive surgical treatment mainly includes endoscopic radiofrequency therapy, endoscopic anti-reflux mucosal ligation, endoscopic anti-reflux mucosal resection, and laparoscopic fundoplication surgery, laparoscopic magnetic ring implantation, etc. Among them, laparoscopic fundoplication can solve both hiatal hernia and esophageal reflux disease. It has the characteristics of less trauma, quick recovery and good curative effect. It is the gold standard for the treatment of hiatal hernia and gastroesophageal reflux disease. Surgery.
At the time of Gastroesophageal Reflux Awareness Week, 9 experts of Gastroesophageal Reflux Disease from the Rocket Army Special Medical Center also sent messages to the general public through this event.
Message from the Experts Poster

Department Profile

Gastroesophageal Surgery, Rocket Army Special Medical Center
The Department of Gastroesophageal Reflux Disease (formerly known as the Department of Gastroesophageal Reflux Disease) of the Rocket Army Special Medical Center was founded in April 2006 by Academician Wang Zhonghao of the Chinese Academy of Sciences. The home gastroesophageal reflux disease center is also the only independent gastroesophageal reflux disease department in the world, with a skilled, responsible and experienced medical and nursing team.
Department has a variety of the most advanced gastroesophageal reflux disease specialist diagnosis and treatment equipment in the world. The main treatment features of the department are laparoscopic fundoplication and micro-radiofrequency treatment of the cardia under gastroscope. At the same time, a variety of anti-reflux techniques have been successively carried out to realize individualized treatment of gastroesophageal reflux disease. The department also conducts minimally invasive treatment of gastroesophageal reflux-related diseases centered on the cardia.
Departments have formed a large-scale and professional effect, and established a standardized diagnosis and treatment process for gastroesophageal reflux disease, so that gastroesophageal reflux disease has gradually been valued by the Chinese and the medical community. Its number of cases, technical strength, academic status, and scientific research achievements are second to none in the country.
This article was first published: Digestive Liver Disease Channel in the Medical Community
This article was written by MSHK
Editor in charge: Wen Jiaxin
Illustration source: too handsome gallery
Copyright Notice
This article is original, please contact for authorization
-End-
The medical community strives for the accuracy and reliability of its published content when it is reviewed and approved, but does not make any guarantees about the timeliness of the published content, and the accuracy and completeness of the cited materials (if any), etc. Any commitments and guarantees, and do not assume any responsibility due to the outdated content, the possible inaccuracy or incompleteness of the cited information. Relevant parties are requested to check separately when adopting or using it as a basis for decision-making.