Source: Shuangyashan Scientific Research Black House
Author: Zhu Que

The athlete’s heart is affected by regular vigorous exercise, with significantly increased hemodynamic demands, and structural and functional adaptive cardiac changes. In general, ventricular dilation, increased myocardial mass, and a decrease in normal resting function measures are common in athletes’ hearts.
However, the biventricular morphology and mechanical characteristics of athletes are affected by multiple factors, such as different training regimes, exercise programs, age and gender , resulting in various adaptive changes. The current cardiac phenotypes of different athletes remain difficult to distinguish, especially with regard to changes in right ventricular adaptation, as most of the current results focus only on the left ventricle.
Furthermore, the physiological link between cardiac remodeling and exercise capacity remains incompletely understood.
Advanced techniques such as deformation imaging and three-dimensional echocardiography have provided more precise and detailed quantification of ventricular structure and function. Deformation along the long axis (via longitudinal strain) is the best measure of ventricular function; however, circumferential strain of left and right ventricular myocardium is also an important physiological component of myocardial contractility.
For different hemodynamic stimuli, ventricular mechanical characteristics can change in a complex manner, which has important diagnostic and prognostic value. Therefore, 3D echocardiography-derived biventricular deformation also helps to reveal the relationship between resting cardiac function and exercise capacity.
In a study published in the European Journal of Preventive Cardiology in February 2022, academics from Hungary exercised heart The medical screening program retrospectively enrolled 425 healthy elite athletes, 304 of whom were members of the national team in the appropriate age group.
All athletes have 3D transthoracic echocardiographic images, detailed medical history, training regimen, standard medical report, twelve-lead ECG data and cardiopulmonary exercise test data. Fifty-five age- and sex-matched healthy volunteers with no exercise habits were included as a control group.
Analyzing this cohort, this study describes the effects of sex, age, and different training modalities on biventricular morphology and function, and the study The relationship between cardiac remodeling and peak exercise capacity.
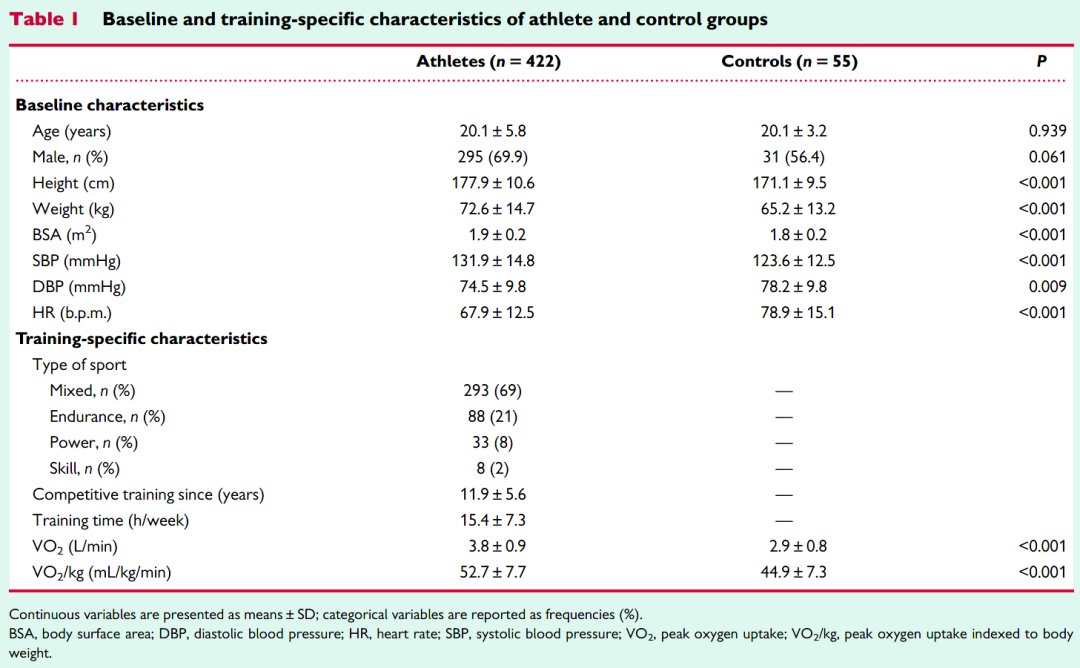
Of the 425 athletes included, most Participated in mixed and endurance sports, mainly water polo (34.8%), soccer (30.6%) and swimming (13.3%). The athletes had higher height, weight and body surface area compared to the control group. The resting systolic blood pressure of the athletes was significantly higher than that of the control group, and the diastolic blood pressure and heart rate were significantly lower than those of the control group.
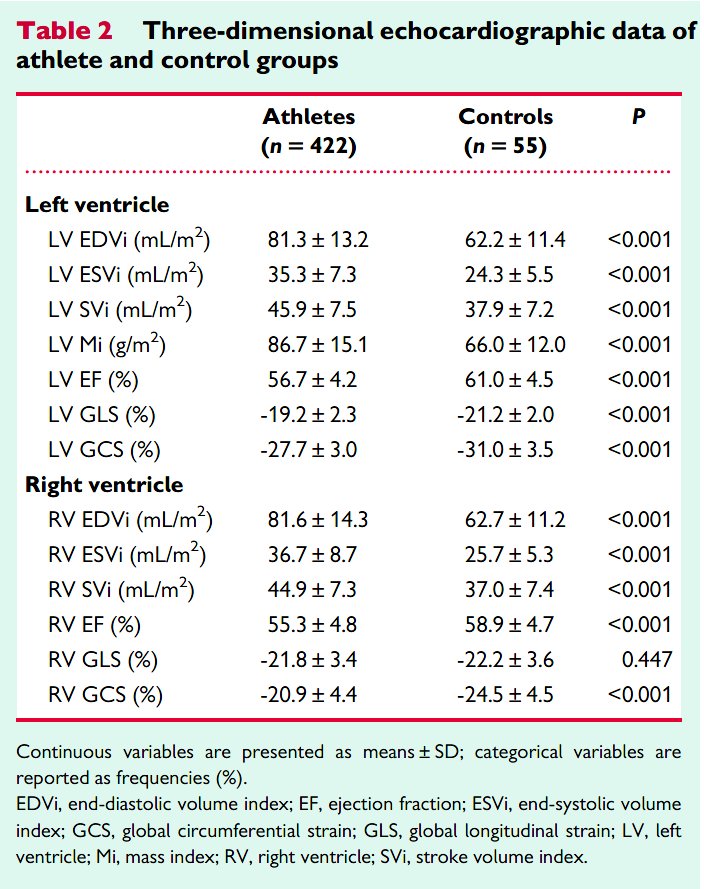
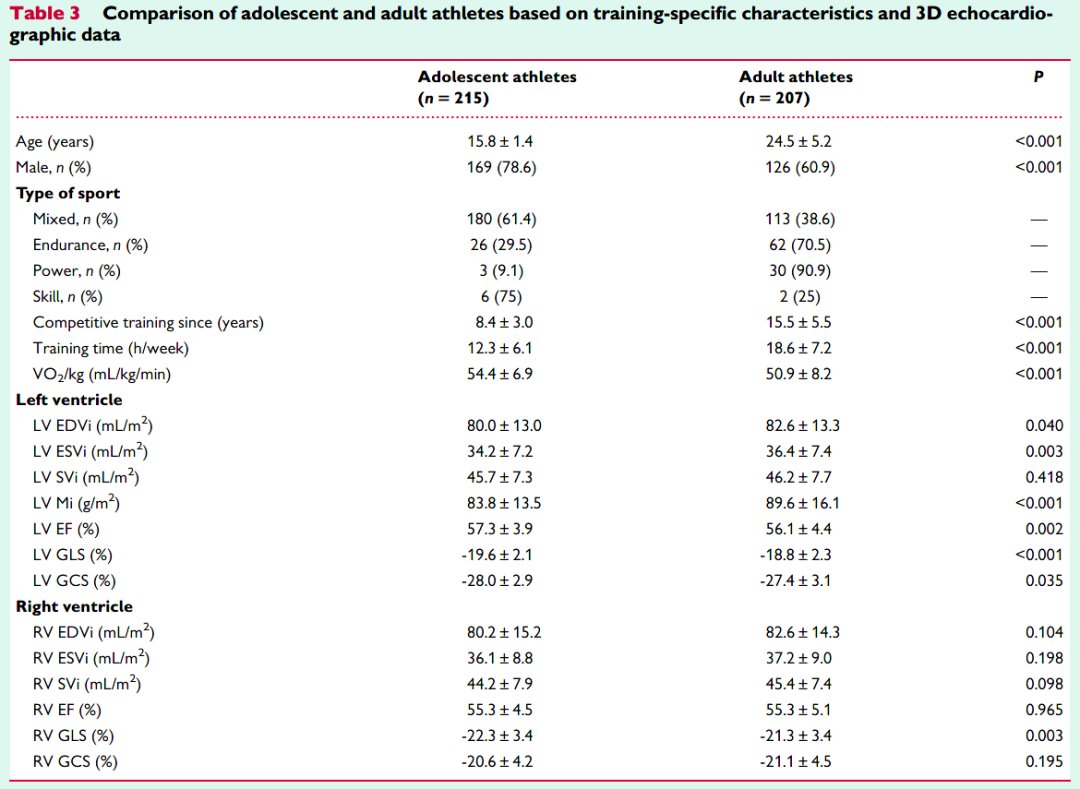
As expected, the athlete and control groups There were significant differences in left and right ventricular morphological and functional parameters. The end-diastolic volume index and end-systolic volume index of the left and right ventricles were significantly higher in athletes.
Similarly, the left ventricular mass index and stroke volume index were higher in the athletes compared with the control group. In athletes, the resting values of LV ejection fraction, LV global long-axis strain, LV global circumferential strain, RV ejection fraction, and RV global circumferential strain were significantly reduced.
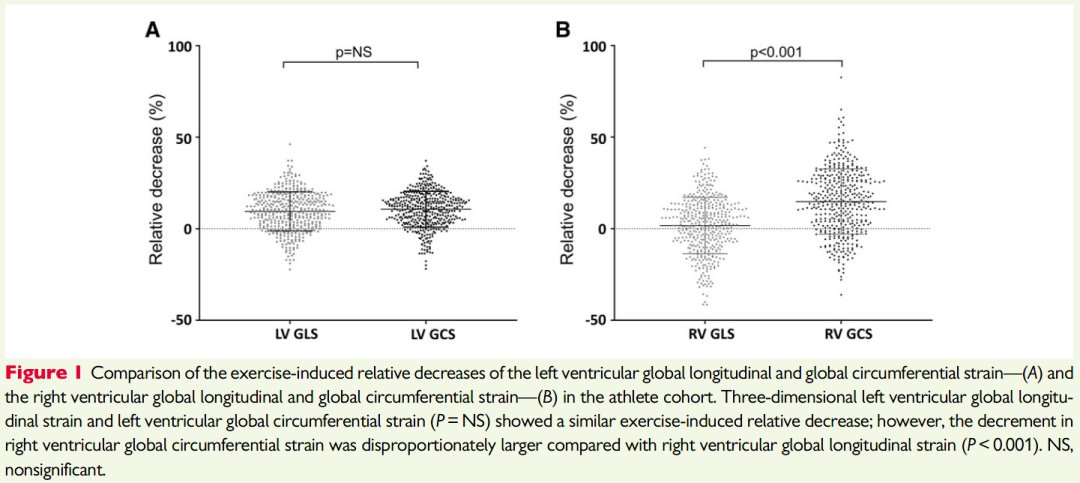
Among athletes, the study also compared exercise The relative reduction in the overall long-axis strain and overall circumferential strain of the left and right ventricles. The overall long-axis strain of the left ventricle decreased by an average of 10% after exercise, and the overall circumferential strain of the left ventricle decreased by an average of 11% after exercise. Degree of decline (2%).
The study also compared different exercise types , including mixed (n=293), endurance (n=88), strength (n=33), and skill (n=8) athletes. Strength athletes exercised the longest, averaging 17 years, while endurance athletes trained significantly longer, averaging 21 hours per week.
Endurance athletes outperformed other groups in peak exercise capacity. Three-dimensional echocardiography showed that the left ventricular cardiac index and left ventricular mass index were significantly lower in strength athletes than in mixed and endurance athletes.
Endurance athletes had the highest RV end-diastolic and RV end-systolic volumes, while strength athletes had the highest RV end-diastolic and end-systolic volumes lower than other groups.
With regard to left ventricular function, global long-axis strain and global circumference of the left ventricle in strength athletes compared with mixed and endurance athletes Strain resting values are low.
In contrast, endurance athletes had the lowest resting values for RV ejection fraction, RV global long-axis strain, and global circumferential strain, while strength Athletes had the highest resting values of RV global circumferential strain.
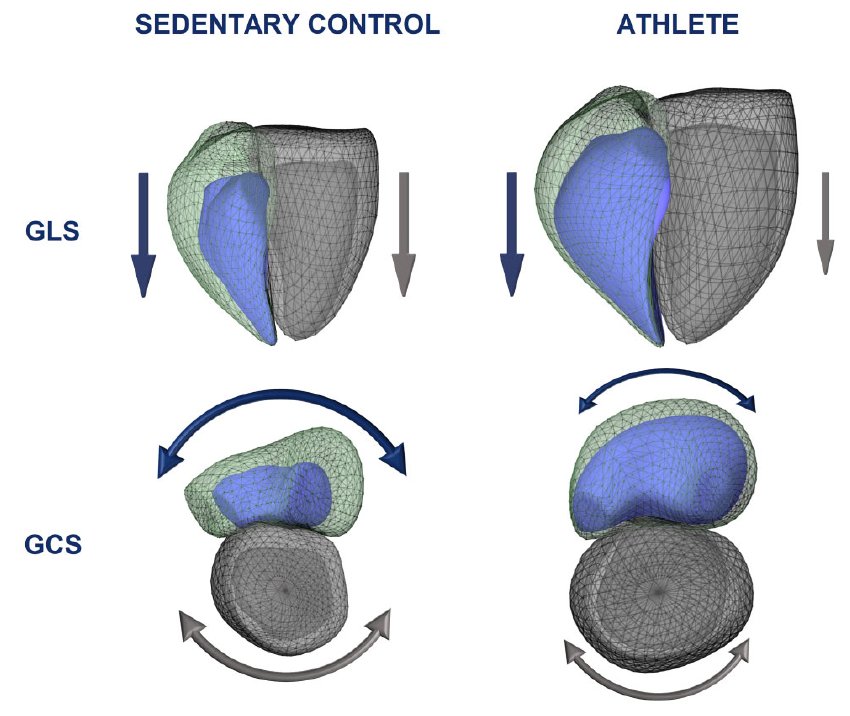
Healthy volunteers and elite athletes in 3D left ventricle and right ventricular volumes and mechanics in terms of graphical representation of left ventricular end-diastolic volume (228 vs. 143 mL), right ventricular end-diastolic volume (237 vs. 139 mL), left ventricular end-systolic volume (104 vs. 42 mL) and right ventricular end-systolic volume (118 vs. 47 mL) were larger.
With regard to systolic function, left ventricular global longitudinal strain values (-20.3 vs. -23.1%) and global circumferential strain values (-25.8 vs. .-33.6%) showed a similar decrease in athletes, while the athletes’ overall circumferential strain of the right ventricle (-12.6 vs. -28.6%), compared with the overall longitudinal strain (-21.1 vs. -25.2%) , showing a disproportionate decrease.
Conclusion
In Athletics In athletes, regular, vigorous physical activity can lead to significant and specific changes in biventricular morphology and function.
Athletes had lower left and right ejection fractions at rest compared to controls. For the left ventricle, the reduction in longitudinal and circumferential shortening was similar; however, the right ventricular circumferential shortening showed a disproportionate reduction.
Our findings underscore the importance of three-dimensional echocardiographic imaging in assessing cardiac function in athletes, understanding normal exercise physiology, and detecting potentially adverse cardiac structures The importance of remodeling.
References
Fábián A, Ujvári A, Tokodi M, Lakatos BK, Kiss O, Babity M, Zámodics M, Sydó N , Csulak E, Vágó H, Szabó L, Kiss AR, Szűcs A, Merkely B, Kovács A. Biventricular mechanical pattern of the athlete’s heart: comprehensive characterization using 3D echocardiography. Eur J Prev Cardiol. 2022 Feb 9:zwac026.