▎WuXi AppTec Content Team Editor
After the beginning of autumn, the autumn wind is gradually rising, and the high incidence of respiratory diseases will soon come. Influenza is an acute respiratory infectious disease caused by influenza virus (influenza A or B virus) infection. The main symptoms include high fever, headache, sore throat, and muscle aches. Influenza not only damages the respiratory system, but also the nervous and cardiovascular systems, and increases the risk of death. The annual seasonal epidemic caused by influenza creates a significant disease burden worldwide.
August 27, 2022, THE LANCET Publishes an Important Symposium Discussion Paper Based on the Latest Research EvidenceEpidemiology, Virology/Onset of Influenza The mechanism, transmission characteristics, clinical symptoms and antiviral treatment are elaborated.
The paper highlights that the prevalence of seasonal influenza has increased significantly over the past two years. Most influenza patients can be relieved within 1 week of symptom onset, but some patients may develop serious or even fatal complications. For those at high risk of influenza complications, we need to pay attention to their treatment and clinical management .
Screenshot source: THE LANCET
Seasonal influenza is an illness caused by human infection with seasonal influenza A or B viruses. Most patients with influenza will have self-limited upper respiratory symptoms, and some patients with influenza (especially young children, the elderly, pregnant women, or patients with certain underlying medical conditions) may develop influenza-related complications and even death in severe cases.
What are the types of flu viruses?
Influenza viruses belong to the Orthomyxoviridae family. Among the 4 different types of influenza viruses (A~D) in the Orthomyxoviridae family, 3 types (A, B, and C) can infect and cause disease in humans.
Influenza A viruses and Influenza B viruses can cause widespread influenza epidemics known as seasonal influenza Virus. Influenza A viruses can infect many birds and some mammals and can cause rare influenza pandemics in humans; influenza B viruses mainly infect humans.
Influenza C viruses can infect humans, pigs and dogs; Influenza D viruses mainly infect cattle but can also spread to other animals. Whether influenza D virus can infect and cause disease in humans is unclear, but related reports have shown that influenza D virus antibodies can be detected in people exposed to cattle.
It should be noted that influenza A viruses are generally divided into different subtypes based on the hemagglutinin and neuraminidase surface glycoproteins. The influenza A viruses currently circulating in the global population are Influenza AH1N1pdm09 virus and Influenza AH3N2 virus. In addition, influenza B viruses circulating in the global population can be divided into two lineages, B/Victoria/2/87 and B/Yamagata/16/88 (since 2020 Influenza B/Yamagata lineage infection has not been reported since March 2009).
The mean intergenerational interval for symptomatic influenza A virus infection was 2.2 days (H3N2) and 2.8 days (H1N1pdm09). In addition, the results of a systematic review showed that the median incubation period of influenza A was 1.4 days and that of influenza B was 0.6 days.
People at high risk for complications from influenza
Influenza virus infection and prevalence rates are highest in children and decrease with age,about 20 % to 40% of the affected population can present with influenza-like illness (fever, cough, or sore throat), while up to half of symptomatic patients have acute upper respiratory symptoms without fever, and approximately 14% of asymptomatic patients % to more than 50%.
The results of a systematic review and meta-analysis indicate that there are more than 32 million cases of influenza-associated lower respiratory tract disease in adults worldwide each year, of which more than 5.7 million adults suffer from Received hospitalization (highest rate for people 65 or older).
Another systematic review showed that in 2018, of the nearly 110 million influenza cases (870,000 hospitalizations) in 5-year-olds worldwide, About 35,000 deaths (more than 15,000 in-hospital deaths) were caused by acute lower respiratory disease.
The paper emphasizes that the influenza epidemic caused by influenza A H3N2 virus is associated with higher morbidity and mortality in the elderly population, and the H3N2 virus undergoes different degrees of antigenic drift. (mutant forms of the influenza virus) are also associated with higher influenza morbidity and mortality in children.
In general,children under 5 years old, elderly people ≥ 65 years old, women within 2 weeks postpartum, immunocompromised people, with certain chronic comorbidities (including lung, Cardiac, neurological, metabolic, hematological disorders, extreme obesity, etc.), and those requiring long-term care are at higher risk for influenza-related complications, which may result in hospitalization and death.
Influenza Symptoms: Complicated and Varied!
In general, seasonal influenza may be clinically manifested by asymptomatic infection, uncomplicated upper respiratory symptoms (with or without fever), and complications, etc. In addition, fever may not be present in many symptomatic patients (especially the elderly and immunocompromised).
Specifically:
Seasonal fluSystemic signs and symptoms include fever, chills, myalgias, malaise, and headache, which usually come on suddenly and are accompanied by respiratory symptoms such as dry cough, sore throat, and runny nose. In addition, ocular symptoms include lacrimation, conjunctivitis, photophobia, eye movement pain, etc., but are relatively rare;
Young children with seasonal flu may also experience gastrointestinal symptoms such as nausea, vomiting, diarrhea, and abdominal pain;
Senior populations with seasonal influenza may also experience systemic symptoms such as malaise, anorexia, dizziness, weakness (without fever), sore throat, and myalgias.
For most people, uncomplicated flu symptoms usually resolve after 3-7 days, but cough and discomfort may persist for more than 2 weeks (especially in older adults and chronic lung disease) population).
Pharmacotherapy and Clinical Management of Influenza
The clinical benefit of antiviral therapy is greatest when antiviral therapy is started immediately after the onset of influenza. Antiviral drugs against influenza A and B viruses include neuraminidase inhibitors and polymerase inhibitors. Among them, neuraminidase inhibitors include oseltamivir, zanamivir, lanimir and peramivir.
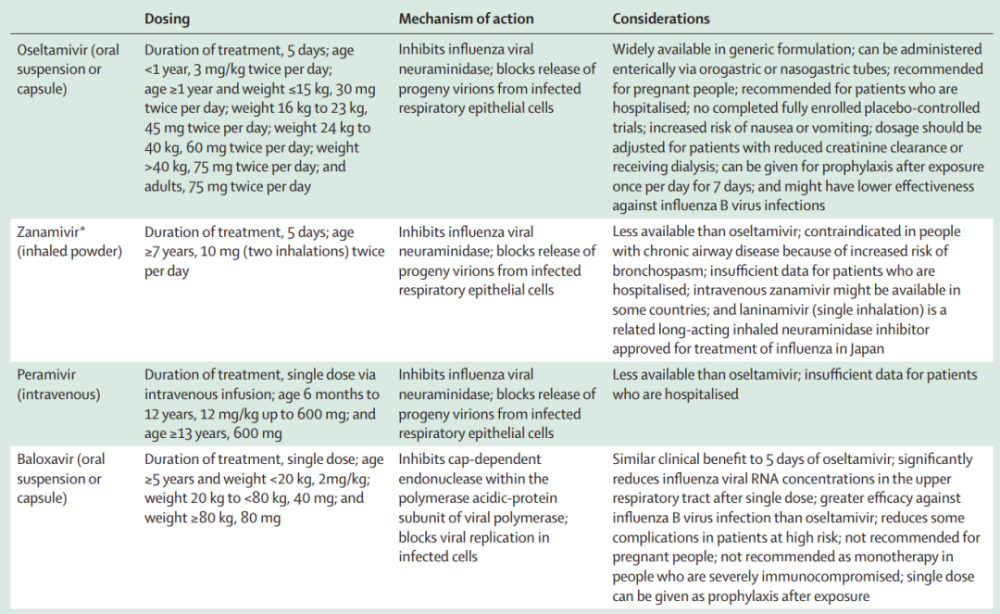
▲Influenza antiviral drugs (Image source: Reference[1])
The paper states that oseltamivir is one of the most widely prescribed neuraminidase inhibitors in the world. A meta-analysis of randomized controlled trials shows that oseltamivir treatment in uncomplicated children with influenza is associated with an overall shorter disease duration compared with placebo About 18 hours (30 hours shorter in those without asthma) and a 34% lower risk of otitis media in patients.
Additionally, uncomplicated adults with influenza who started oseltamivir within 36 hours of symptom onset were patients less likely to suffer from symptoms compared to placebo Median time to remission was reduced by 25 hours, the risk of lower respiratory tract complications (which occurred after 2 days of oseltamivir treatment and required antibiotics) was reduced by 44%, and the risk of hospitalization for any reason was reduced by 63%.
The paper pointed out that At present, the use of M2 ion channel protein inhibitors such as amantadine and rimantadine is not recommended for the treatment of influenza A and B virus infections. On the one hand, these drugs have no antiviral activity against influenza B virus; on the other hand, these drugs have a high resistance rate in influenza A virus.
In general, for patients with influenza who do not require hospitalization, antiviral therapy should be started as soon as possible after illness onset (especially those at high risk of complications from influenza or those with progressive disease) ) and supportive care. In addition to prompt initiation of antiviral therapy and infection prevention and control measures for hospitalized patients, the clinical management of influenza should involve supportive care for complications (eg, antibiotics for bacterial co-infections). treatment or low-flow auxiliary oxygen supply, etc.), and take effective measures to prevent the deterioration of related chronic diseases.