Pediatric skin has always been a common disease in pediatric internal medicine, but due to the specialization of the surgery industry, more and more related diseases are involved in pediatric internal medicine. “Diagnosis and treatment” and lost his own knowledge and cognition of children’s skin.
Acute pityriasis lichenoides acnes is an erythematous scaly disease of unknown etiology that has a rapid onset and can occur in all age groups.
Case review
Children, female, 4 years old, mainly because of “repeated rash all over the body for more than 7 months, aggravating for 3 months”.
The mother of the child complained that the child had fever without obvious incentives before 7 months, the highest body temperature could reach 38.0 ℃, and several soy-sized skin color papules appeared on both lower extremities and the inside of the toes, and there was no obvious self-consciousness. symptom.
Go to the local county hospital and take oral “Four Seasons Antiviral Oral Liquid, Loratadine” (the specific dose and usage are unknown) for half a month, no improvement, and rash Gradually increased, and involved the buttocks, and continued to receive “antiviral and antiallergic” treatment at the local city hospital.
Before 3 months, the rash of the child increased significantly and spread all over the body, especially on both upper limbs. The rash was mainly distributed in dense and symmetrical, non-integrated, red, skin-colored papules, papules, Necrosis, crusting, and desquamation were seen in individual rashes, and the patient was referred to our hospital.
Initial diagnosis: Acute pityriasis lichenoides pimples
Physical examination on admission: The general condition is good, the examinations of various systems are normal, the superficial lymph nodes of the whole body are not palpable and enlarged, and the examination of the heart, lung and abdominal system is unremarkable Obviously abnormal.
Dermatological examination: The face, trunk, extremities, hands, and feet can be seen with multiple reddish or reddish-brown, miliary to broad bean-sized macules, papules, papules , Pigmentation and hypopigmentation spots, densely distributed, not integrated with each other, some scales on the surface of some rashes, triad of psoriasis (-), necrosis and crusting on the surface of individual papules, no tenderness, bleeding and secretions. The oral and genital mucosa were not involved.
*Note
The triad of psoriasis:Silver scales, spotting, film
Laboratory and auxiliary tests:
Blood routine: neutrophil ratio 0.22, lymphocyte ratio 0.69, absolute neutrophil value 1.02×10^9/L, cytomegalovirus IgG antibody 53.112 AU/mL.
Weakly positive for Mycoplasma pneumoniae IgM antibody.
Analysis of lymphocyte subsets: B lymphocytes CD3-CD19+: 24.4%, NK cells CD3- CD56+: 2.5%, Epstein-Barr virus antibody IgG and IgM, urine routine, liver and kidney function, biochemistry are normal.

The picture is from this case
Treatment
Intravenous after admission: Compound Ammonium Glycyrrhizinate Injection 40 mg/time, once daily, Clindamycin Phosphate Injection 0.2 g/time, bid, orally Levoxacin Tirizine oral liquid 3 mL/time, 2 times/d, topical mometasone furoate cream (trunk and limbs) 2 times/d, 0.03% tacrolimus ointment (face) 1 time/d.
After 10 days of treatment, the rash basically subsided and no new rash was seen. The discharge was instructed to be given “Erythromycin 75 mg/time 3 times/d, Compound Glycyrrhizin Tablets 1 tablet/time tid “oral.
Follow-up
During the regular monthly follow-up and follow-up, the children occasionally had new skin lesions without obvious incentives. In the most severe cases, rashes appeared in batches, manifested as red papules with flushing around them. The rash appeared necrotic and crusted. After 6 months of follow-up, the patient basically recovered, leaving pigmentation, crusting and acne-like scars.

Image from this case: scattered hyperpigmented spots, hypopigmented spots, atrophic acne scars on trunk and extremities
Knowledge extension
Characteristics of acute pityriasis lichenoides rash
01. The skin lesions have pleomorphic changes: erythema, papules, maculopapular rashes, blisters, pustules, necrosis, crusts, etc., which can be left after healing Lower acne-like scars;
02.No symptoms: Because the rashes appear in batches, rashes at different stages of development can be seen at the same time;
03. The rash is generalized: mainly on the trunk, abdomen and upper arms, especially on the flexor side, palms, toes and face are rarely involved, sometimes oral and genital mucosal lesions are seen, and the lesions are generally limited It does not affect the health of the whole body.
Differential diagnosis of acute acne pityriasis lichenoides rash
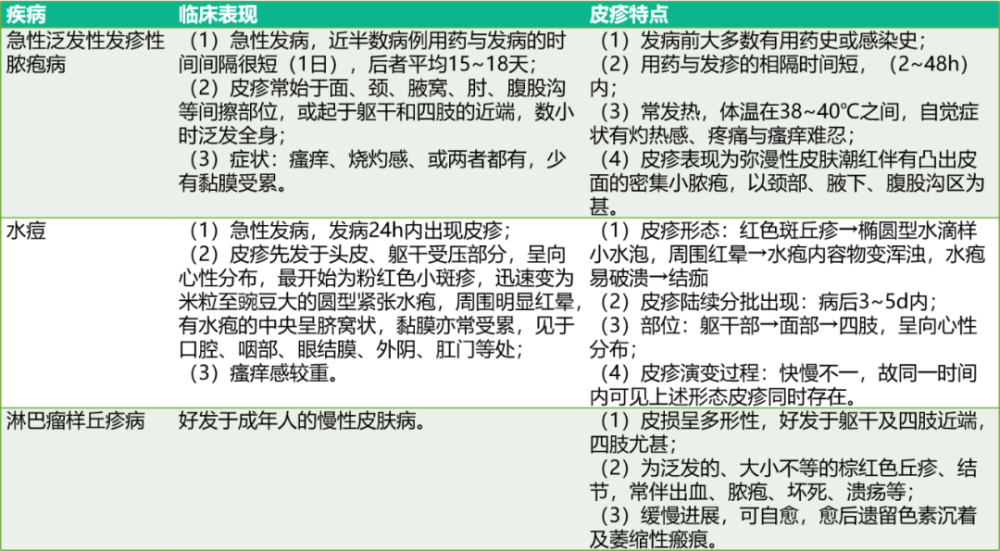
Differential Diagnosis Picture
01.Acute generalized exanthematous pustulosis

Image source: Mai T.C.C., Vo T.T.V., Nguyen T.T.M., Le T.C.N., Nguyen T.T.P., Pham T.N., Mai B.H.A. 2021. A ten-day-old newborn with acute generalized exanthematous pustulosis. Eur . J. Pediat. Dermatol. 31(2):87-90. 10.26326/2281-9649.31.2.2234.
02.Chickenpox

Image source: https:https://www.healthline.com/health/chickenpox
03.Lymphomatoid papulosis

Image source: A case of lymphomatoid papulosis in children [J], Journal of Dermatology and Venereology, 2018, 6(25)3.
Acute acne-like pityriasis lichenoides treatment
01. At present, there is no uniform standard for this disease, and there are currently effective treatments for this disease, including topical therapy (glucocorticoids and calcineurin inhibitors) ), systemic drugs (antibiotics and immunosuppressants such as methotrexate, cyclosporine, dapsone, etc.) and phototherapy;
02.Erythromycin and tetracycline: Erythromycin 10 mg/kg/d is more suitable for children, and tetracycline is more suitable for adults; p>
03. Ultraviolet rays: commonly used in clinical treatment, but after stopping phototherapy, the disease recurs without obvious incentives; side effects include: erythema, itching, burning, stinging, hair follicles inflammation, headache and dryness.
Planning: Zhang Jie
Title image: Zhanku Hailuo
[1] SKINNER B, LEVY A L. Rapid resolution of pityriasis lichenoides et varioliformis acuta with azithromycin[J]. J Am Acad Dermatol, 2008, 58(3): 524-525;
[2] BELLINATO F, MAURELLI M, GISONDI P, et al. A systematic review of treatments for pityriasis lichenoides[J]. J Eur Acad Dermatol Venereol, 2019, 33(11): 2039-2049.3] Liu Dongyan, Wang Tingting, Yi Qin. A case of acute acne-like pityriasis lichenoides and literature review[J]. Sichuan Medicine, 2021, 42(1): 104-106.
[4] Xie Xiaolei, Wu Yuan, Song Yingjie, etc. A case of acute acne-like pityriasis lichenoides [J]. Chinese Journal of Leprosy and Dermatology, 2017, 33(6): 355-356.
[5] JUNG F, SIBBALD C, BOHDANOWICZ M, et al. Systematic review of theefficacies and adverse effects of treatments for pityriasis lichenoides[J].Br J Dermatol,2020,183( 6) : 1026-1032.