For medical professionals only
A comprehensive interpretation of HPV and TCT
In cervical cancer screening, the two most frequently performed tests are HPV and TCT. So, how to understand these two reports?
To understand the report of an HPV test, we must first know what it checks.
HPV test
HPV, short for Human Papillomavirus, is believed to be the culprit behind cervical cancer. HPV is a large family, and more than 120 kinds of HPV have been found so far, among which there are 14 kinds of high-risk HPV. HPV testing is to see if there is HPV, especially high-risk HPV and highest-risk HPV infection.
The report form of HPV test is generally divided into two categories: simple and detailed.
The detailed HPV test report will list each HPV tested and tell you whether it is negative or positive one by one, and some test report results are not represented by negative or positive, but If a value is given, there will be a reference range at the back. Generally, those within the reference range are negative, and those beyond the reference range are positive.
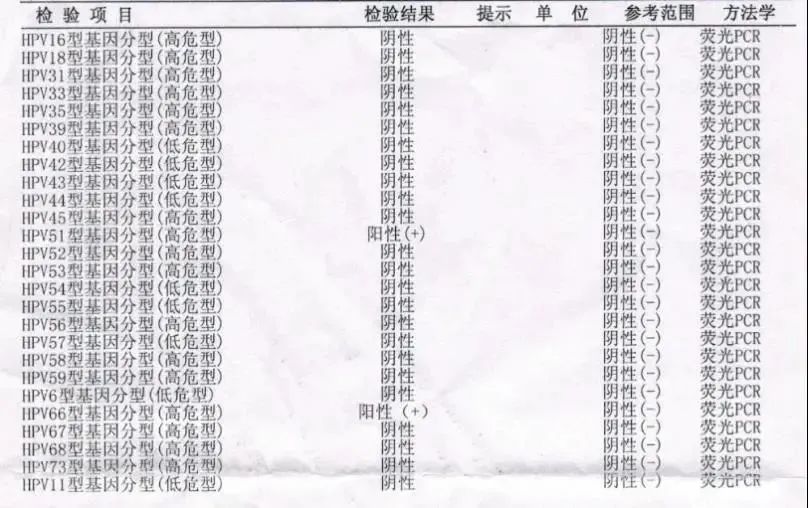
The simple HPV report is to directly package the high-risk and highest-risk HPV results together. If the packaged result is negative, it means that these types of HPV are not available.
Does a positive HPV test mean cervical cancer?
Of course not!
HPV infection is the main risk factor for cervical lesions, but it does not mean that HPV infection will definitely lead to cervical lesions, and it needs to be further clarified with cervical cytology (TCT).
TCT Check
As with the HPV test, let’s take a look at what the TCT checks.
TCT stands for “thin-layer liquid-based slice cytology test”, which is the most advanced cervical cancer screening technology in the world. The images produced by the thin-layer liquid-based preparation technique have a clear background and sufficient and uniform cells, which greatly improves the accuracy of cytology. In one sentence: Let me see if you (cervical cells) are developing normally!
Take this inspection report as an example to expand the description-
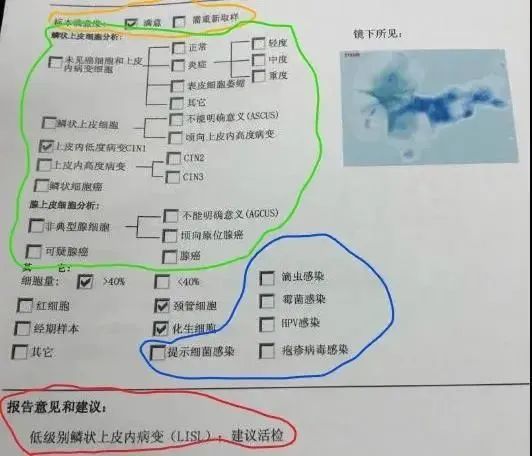
In general, a TCT report can be divided into the following parts:
1
Specimen Satisfaction
That is, the part circled in orange, divided into satisfied and dissatisfied. Unsatisfactory specimens require resampling.
2
cervical microbiome
That is, the part circled in blue in the above picture, TCT examination can not only screen for cervical cancer, but also detect trichomoniasis, mold and other pathogenic microorganism infections. If there is an infection, the doctor will tick the corresponding pathogen.
3
Cell specific diagnosis
That is, the part circled in green in the above figure is divided into the analysis of squamous epithelial cells and the analysis of glandular epithelial cells. Some reports do not have this section or are only included in one pass.
Analysis of squamous epithelial cells was divided into no intraepithelial lesions, atypical squamous cells, low-grade intraepithelial lesions, high-grade intraepithelial lesions, and squamous cell carcinoma ranging from mild to severe There are several levels, each with a specific description behind it. The description of glandular epithelial cells is divided into atypical glandular cells, suspicious adenocarcinoma, adenocarcinoma and other levels.
4
Report comments and suggestions
The fourth part is the important part and the part we pay attention to first, which is the part circled in red in the above picture: report comments and suggestions. Some results may appear in this section:
(1) No intraepithelial lesions or malignant lesions (NILM) are found. If the HPV test is done at the same time and the result is negative, it means that no cervical lesions are found, and regular review is enough; if HPVIf high-risk HPV is found in the examination, it needs to be re-examined 6 to 12 months later. If it is positive for the highest-risk HPV, further colposcopy and cervical biopsy may be required.
(2) Atypical squamous cells (abnormal squamous cells) include:
①Atypical squamous cells of no clear significance (ASC-US).
②If atypical squamous cells (ASC-H) of high-grade squamous intraepithelial lesions cannot be excluded, further examination by colposcopy is often necessary.
(3) Low-grade squamous intraepithelial lesion (LSIL): It indicates abnormal cells and requires further colposcopy and biopsy of suspicious lesions.
(4) High-grade squamous intraepithelial lesion (HSIL): Indicates that there are suspicious precancerous cells and needs further diagnosis and treatment, otherwise it is more likely to develop into cancer. If HPV is not checked, the doctor will ask you to check for high-risk HPV, and at the same time, perform colposcopy + cervical biopsy as soon as possible, and perform cervical conization according to the degree of the lesion.
(5) Atypical glandular epithelial cells (AGC): It is very likely to be a precancerous lesion. At this time, further examination to be done is not limited to the cervix, but also includes the endometrium . The doctor will recommend colposcopy + cervical biopsy + cervical scraping and curettage as soon as possible to confirm the diagnosis, and if necessary, diagnostic curettage or hysteroscopy to exclude endometrial lesions.
(6) Squamous epithelial carcinoma (SCC) or adenocarcinoma: This indicates that the cervix has become cancerous, and multiple cervical biopsy under colposcopy should be performed in time, seek medical attention in time, and treat as soon as possible.
It is important to remind everyone that you should not think that you can make a diagnosis by yourself if you have this knowledge. The diagnosis should still be done by a professional doctor. After all, HPV and TCT are relatively primary diagnoses in the cervical cancer inspection system. To make an accurate judgment, further colposcopy and pathological biopsy are required.
The source of this article: Red House Hospital Patient Mobile Service Platform
Editor in charge: Yi Chuan