Potassium ion is one of the most important cations in the human body. More than 98% of potassium in the human body is located in the cells. Potassium ions are directly involved in metabolic activities inside and outside cells, including maintaining cell metabolism, regulating osmotic pressure of body fluids, maintaining acid-base balance and maintaining cellular stress functions.
Under normal circumstances, the concentration of serum potassium ion (blood potassium) is 3.5~5.5mmol/L, when serum potassium is >5.5mmol/L, it is excluded from laboratory test errors or hemolysis, etc. Hyperkalemia can be diagnosed after pseudohyperkalemia. According to data, the prevalence of hyperkalemia in the general population is about 2% to 3%. Although people with mild hyperkalemia are usually asymptomatic, severe hyperkalemia can lead to cardiac arrest, muscle weakness or paralysis, or even life-threatening. This article mainly introduces the etiology, clinical manifestations and clinical treatment of hyperkalemia.
One. Symptoms of hyperkalemia
The causes of hyperkalemia are complex, and common risk factors include heart failure, kidney disease, and the use of certain medications. Hyperkalemia is divided into mild, moderate and severe according to serum potassium concentration. The serum potassium concentration of mild hyperkalemia is 5-5.5 mmol/L, the serum potassium concentration of moderate hyperkalemia is 5.6-6.0 mmol/L, and the serum potassium concentration of severe hyperkalemia is >6.0 mmol/L.
The higher the potassium level, the greater the life-threatening risk. Severe hyperkalemia can affect muscle function in the extremities and even lead to cardiac arrest. Extracardiac manifestations can be manifested as increased neuromuscular excitability, loss of muscle cell excitability, and central nervous system manifestations of restlessness and confusion.
The main impact on the heart is arrhythmia, which can be clinically various bradyarrhythmias, such as atrioventricular block, sinus bradycardia, etc.; Disorders such as sinus tachycardia, frequent premature ventricular contractions, ventricular tachycardia, and ventricular fibrillation. The ECG changes of hyperkalemia include high peak of T wave, shortening of Q-T interval, gradual widening of QRS wave with decreasing amplitude, and gradual disappearance of P wave shape. In addition, the ECG changes of hyperkalemia may not be completely parallel to the serum potassium level, and a small number of patients have sudden death without ECG prodromal manifestations.
In addition, hyperkalemia can cause gastrointestinal symptoms such as nausea, vomiting, and abdominal pain due to increased acetylcholine release. Therefore, early identification and treatment of hyperkalemia can save lives.
The etiology of hyperkalemia
The causes of hyperkalemia generally include excessive intake, decreased excretion, and altered distribution. In addition, the application of certain drugs can also affect potassium balance, which can lead to hyperkalemia.
1) Excessive intake:
Normal intake of potassium-rich foods usually does not cause hyperkalemia, but in people with kidney disease, high intake of potassium-rich foods, foods that are low in sodium and high in potassium Salt substitutes, nutritional products with high potassium content and additives, due to impaired renal function, the ability to excrete potassium is reduced, and hyperkalemia is prone to occur.
In addition, the infusion of potassium-containing drugs, such as penicillin, carbenicillin, and rapid and large blood transfusions, especially bank blood transfusions, can lead to elevated serum potassium, which may lead to hyperkalemia.
2) Reduced excretion:
The kidneys are the main organ that excretes potassium, and in chronic renal failure, the glomerular filtration rate decreases and potassium excretion is markedly reduced, leading to hyperkalemia. As the glomerular filtration rate continued to decline, the incidence of hyperkalemia increased significantly. In addition, the excretion of potassium is also regulated by hormones such as plasma aldosterone and cortisol. When hyporenin-induced hypoaldosteronism, renal tubular acidosis, and azotemia occur, it can cause increased renal tubular potassium recovery and reduced potassium excretion.
Also, cardiovascular disease, especially heart failure, can induce hyperkalemia due to decreased renal perfusion. Long-term use of potassium-sparing diuretics (spironolactone, triamterene) and other drugs that reduce potassium excretion (ACEI, heparin, non-steroidal anti-inflammatory drugs) can cause increased renal tubular potassium recovery and reduced potassium excretion.
3) Distribution changes:
such as tissue damage (crush syndrome, muscle contusion, hemorrhage, etc.), tissue hypoxia, drugs (beta-blockers, alpha-agonists, succinylcholine, digitalis poisoning) and acidosis, which lead to the distribution of intracellular potassium ions to the outside of the cell.
Third, treatment of hyperkalemia
The treatment of hyperkalemia is based on the treatment of the cause and emergency treatment to prevent the occurrence and progression of fatal complications.
Treatment options include:
1) Stabilize the myocardium and relieve the toxicity of potassium ions to the myocardium;
2) Promote the entry of potassium ions into cells and reduce serum potassium levels;
3) Promote the excretion of potassium ions from the body and reduce the total potassium content in the body;
Although the implementation of this series of treatment measures can effectively reduce the potassium ion concentration in extracellular fluid; however, specific clinical decision-making needs to be carried out according to certain ideas.
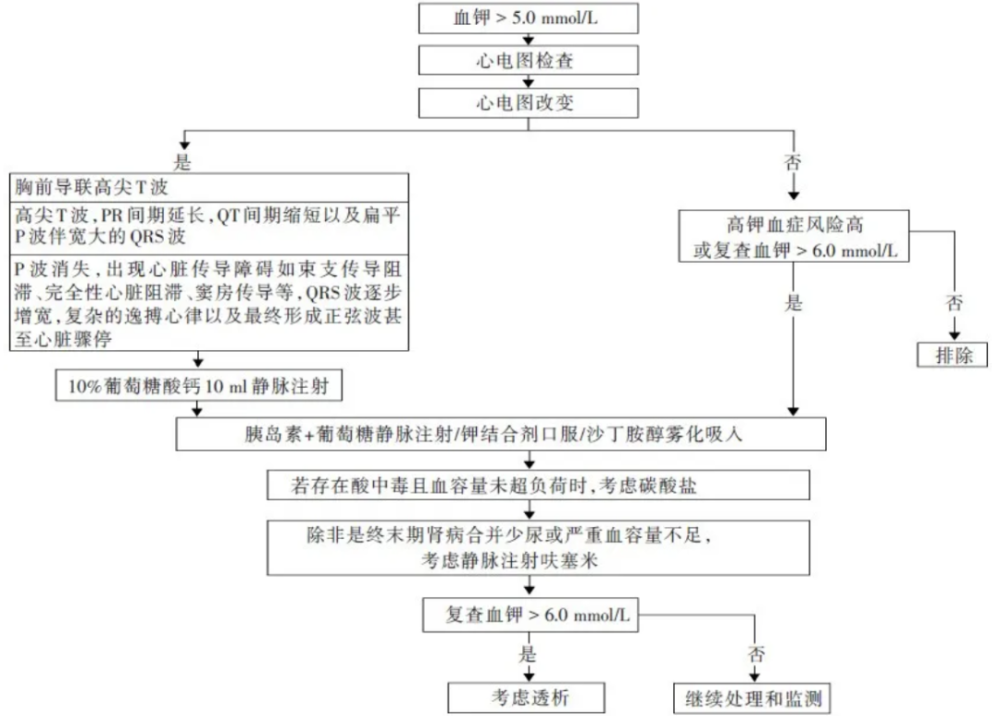
Acute hyperkalemia management process.
Step 1: Stabilize the myocardium
In patients with hyperkalemia with or without ECG changes, use intravenousPulse calcium is the first-line treatment option. Calcium ions can quickly counteract the effect of potassium ions on myocardial action potential, stabilize the cell membrane potential, and restore the excitability of cardiomyocytes to normal.
How to use: Commonly used 10% calcium gluconate solution 10~20ml, diluted and slowly injected intravenously under ECG monitoring, no less than 5 minutes, within 3 minutes Can effectively improve poor ECG performance. If there is no significant improvement in the ECG after 10 to 20 minutes or the abnormality reappears, the dose can be repeated.
Notes:
1) Because calcium ions can aggravate the cardiotoxicity of digitalis, those who use digitalis drugs should be used with caution.
2) Calcium gluconate is less irritating to the vein and can be injected through a peripheral vein. However, large doses of calcium chloride may cause tissue necrosis, so central vein infusion is required.
Step 2: Promote the entry of potassium ions into the cell
1) Glucose + Insulin
Intravenous insulin + glucose can lower blood potassium levels by promoting potassium ion transport into cells.
How to use: 10% glucose solution 500ml+10 IU regular insulin intravenous drip for more than 1 hour. Generally, the onset of effect is 10 to 20 minutes after injection, the peak is 30 to 60 minutes, and it is maintained for 4 to 6 hours, which can reduce serum potassium by 0.6 to 1.0 mmol/L.
Notes:
1, in case of patients with heart failure or oliguria, the infusion rate should be slow;
2, if you want to limit the water intake, you can increase the glucose concentration to 50%, and adjust the insulin dosage according to the blood sugar level;
3, closely monitor the changes in serum potassium and blood sugar during the infusion process to avoid hypoglycemia;
2) Sodium bicarbonate
If the patient has metabolic acidosis, sodium bicarbonate can be injected intravenously to promote the entry of potassium ions into the cells through H+-Na+ exchange.
How to use: 5% sodium bicarbonate 150~250ml intravenous drip, effective within 5~10 minutes and lasts about 2 hours.
Notes:
1, because sodium ions may increase the volume load in patients with CKD, it should be used with caution in patients with concomitant heart failure.
2. Compared with other potassium-lowering regimens, sodium bicarbonate monotherapy does not significantly reduce serum potassium.
3) β-adrenergic receptor agonists
Albuterol combined with insulin-glucose is more effective than either alone.
How to use: 10~20mg salbutamol spray can reduce blood potassium concentration by 0.5~1.5mmol/L within 30~60min, usually take effect within 30 minutes, Lasts about 2 hours.
Notes:
1. Because salbutamol is more effective in combination with high-glucose insulin, it is not suitable as a single drug for patients with severe hyperkalemia.
2, the potassium-lowering method only works for a few hours, and cannot expel potassium ions, which is prone to rebound.
Step 3: Promote the excretion of potassium ions from the body
1) Diuretics
It has limited effect in patients with severe chronic kidney disease, but is more effective in patients with low renin and low aldosteronemia. Combination of loop diuretics and thiazide diuretics is more effective, but in patients with hypovolemia, it may reduce the glomerular filtration rate, affect renal function and aggravate hyperkalemia.
2) Cation exchange resin
Cation exchange resins reduce the absorption of potassium ions by exchanging sodium or calcium ions for potassium ions in the colon and facilitate their excretion in the feces. At present, sodium polystyrene sulfonate (SPS) and calcium polystyrene sulfonate (CPS) are commonly used in clinical practice, and Patiromer is a new type of ion exchange polymer. These drugs are prone to cause constipation, and there is a risk of intestinal obstruction and intestinal perforation.
3) New potassium ion binding agent sodium zirconium cyclosilicate
In the whole intestine, it captures potassium ions with high selectivity by replacing sodium/hydrogen ions, reducing the absorption of potassium ions in the intestines, thereby quickly and effectively reducing blood potassium concentration.
4) Dialysis treatment
Dialysis therapy is the preferred option for the management of severe hyperkalemia, especially in patients with uremia and existing vascular access. Hemodialysis has a better potassium-lowering effect than peritoneal dialysis, and continuous renal replacement therapy (CRRT) is used more in patients with hemodynamic instability.
IV. Hyperkalemia therapyManagement
After treatment for hyperkalemia is stabilized, further steps should be taken to prevent recurrence of hyperkalemia, especially in elderly patients and patients on hemodialysis. Management measures mainly include identifying and correcting the triggers of recurrent hyperkalemia, dietary control, reducing potassium ion intake, drug intervention and so on. In addition, for high-risk patients, real-time monitoring of serum potassium changes should be performed, and the frequency of serum potassium monitoring should be increased to detect abnormal fluctuations in serum potassium in time.
In conclusion, hyperkalemia is a common and sometimes insidious clinical emergency with a high risk of death. Clinically, in the face of hyperkalemia, the degree of urgency should be determined first, and effective treatment should be carried out. During the treatment process, the dose and speed should be administered in strict accordance with the instructions, and the changes in electrocardiogram and other vital signs should be closely observed.
References:
1. Heart Failure Professional Committee of Chinese Medical Doctor Association. Expert consensus on ion management for patients with heart failure in China [J]. Chinese Journal of Heart Failure and Cardiomyopathy, 2020(01):16-31.< /p>
2. Expert Group of Nephrology Branch of Chinese Medical Association. Expert consensus on the practice of serum potassium management in patients with chronic kidney disease in China [J]. Chinese Journal of Nephrology, 2020,36(10):781 -792.
3.Stefano Bianchi1 et al.Management of hyperkalemia in patients with kidney disease: a position paper endorsed by the Italian Society of Nephrology[J].Journal of Nephrology,2019,32:499- 516.
Source | New Frontiers in Cardiovascular at Mace
Writing |samll year & rayms
Edit | Yanyan