The most critical and dangerous thing in chest pain is cardiovascular disease. Therefore, it is right to seek cardiologist first for chest pain, and cardiovascular emergencies should be ruled out first. However, there are many other causes of chest pain.
This child is just that.
A 17-year-old high school student suddenly had severe left chest pain 10 days ago. After telling his parents, he rushed to the hospital.

I went to the emergency department to check the electrocardiogram, heart ultrasound, and chest CT, but no problem was found, but the blood myocardial enzyme, scientific name “phosphocreatine kinase isoenzyme”, was slightly elevated. High, a little higher than the normal value, the three items of myocardial infarction are also normal, the myocardial injury marker “troponin” is not high, and other related coagulation indicators are also normal. In this way, acute myocardial infarction is not supported, nor aortic disease, pericardial disease, cardiovascular diseases that can cause chest pain.
No major heart problems are found, check your breathing!
Because no substantial lesions were found in the lungs by chest CT examination, the Department of Respiratory Medicine performed pulmonary function tests on the patient. Results When the pulmonary ventilation function was examined, it was found that the airway resistance increased. Will there be bronchospasm? Although bronchospasm and severe chest pain are not consistent, but the problem was found to be further checked, so a methacholine challenge test was performed, and the result was negative, indicating that there was no airway hypersensitivity, no bronchospasm, or asthma.
However, the patient still has chest pains, which are obvious in the upper left chest.
Ten days later, the parents brought their children to the Cardiology Clinic again.
*Ask medical history.
That’s what happened before. To identify, you need to understand the situation of the chest pain attack.
Chest pain is a sudden, tearing sensation while sitting still. Sudden tearing chest pain, it is easy to think of aortic disease, such as aortic dissection. The onset of the disease at rest is not very supportive, and the shape of the aorta is normal as seen by chest CT. Although the CT scan is a plain scan, no medicine is used, but the initial screening is possible.
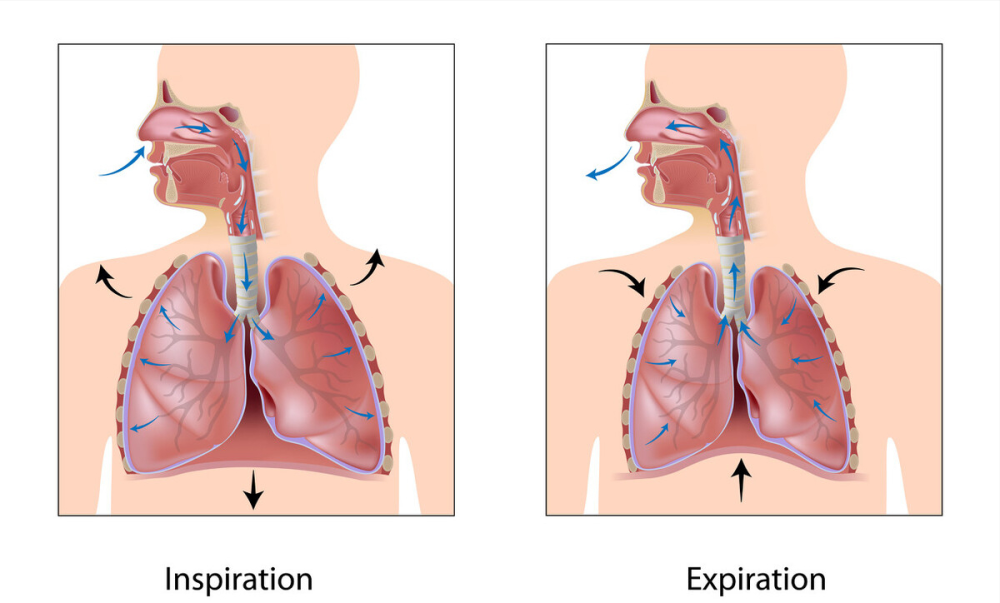
Is chest pain related to breathing? Breathing pain? Painful breathing?
Breathing pain! It hurts when you breathe in.
Sudden chest pain that persists for 10 days, related to breathing, and worsens on inspiration, evoking pleural lesions. Pain occurs when the pleura is stretched and stimulated during breathing. It should also be a respiratory disease. Although no abnormalities were found on chest CT, it may have been a timing issue.
* Check it out.
Slim body, flat thorax, no abnormal chest skin appearance, no tenderness, excluding chest pain caused by skin lesions such as herpes zoster; no tenderness in the sternum and ribs, Chest pain caused by costochondritis, chest wall soft tissue damage, etc. is also not supported; heart sounds are normal, except for slightly lower lung breath sounds, no wet or dry rales are heard.
* Further inspection.
Recheck ECG; chest CT has been checked, a chest X-ray; Myocardial enzymes have been slightly increased, recheck strong>Let’s check the myocardial injury marker troponin again, because the window period is long, if there is a problem, it can be changed within 10 days.
* A chest X-ray provides the diagnosis.
Small pneumothorax in left lung! The gas is in the upper left chest, at the apex of the lungs, with very little compression in the lungs.
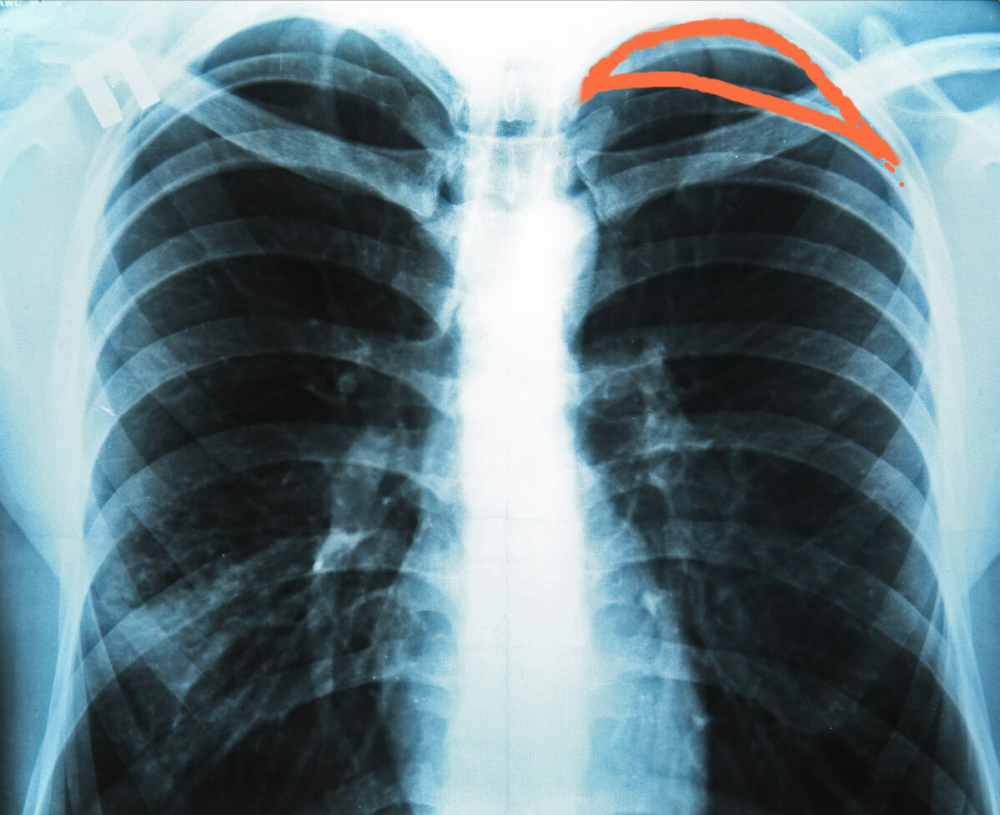 Find a similar picture and draw a diagram
Find a similar picture and draw a diagram
This will explain the patient’s sudden, tearing sensations, left chest pain related to breathing, and the patient is slender and slender, with a flat thorax, which is also a body type prone to pneumothorax. Such people are prone to lesions in the alveoli, and are prone to rupture when the pleural pressure suddenly increases such as coughing, breath-holding, and shouting, resulting in pneumothorax. Pneumothorax can also occur in a resting state. This type of pneumothorax is called “spontaneous pneumothorax”.
Generally speaking, during pneumothorax, the lung compression is less than 30%, no special treatment is required, and the gas will be absorbed by itself. The patient has been treated in the respiratory department and will go to a follow-up consultation.
At the end of the day, some people may say that it was enough to take a chest X-ray at the beginning, and there were so many checks. This is in hindsight, and in hindsight, of course, everything is clear. But when a patient with sudden severe chest pain came to the clinic, he must have thought that cardiovascular disease must be ruled out first, because it is the most dangerous and deadly. The chest CT examination of pneumothorax is also a good imaging technology, but it was not detected in this patient. This is because there are some limitations in various imaging techniques, and it is impossible to achieve a 100% detection rate. A study reported that the coincidence rate of spiral CT diagnosis of pneumothorax with clinical and thoracoscopy was 88%. , Moreover, the patient’s pneumothorax gas volume is relatively small.
There are many reasons for chest pain. Doctors are like detectives. It is a process of continuous analysis and identification.
(All rights reserved, do not reprint without my authorization!)