*For medical professionals only
How to choose human albumin for efficient volume expansion?
Albumin Jun: “Intravenous fluid resuscitation is a common treatment for hemodynamic instability in intensive care unit (ICU) patients. However, due to increased capillary permeability, fluid extravasation As well as the accumulation of body fluids in tissues and other reasons, early volume expansion is sometimes not easy to fully exert its beneficial effects[1-2].
The literature shows that compared with crystalloids, human albumin solution resuscitation can better maintain plasma colloid osmotic pressure and produce greater volume expansion effect [3-5]. Today, Albumin Jun will take a look at the physiological effects and safety of low-dose fluid resuscitation with 20% to 25% of human serum albumin in critically ill patients. “
less fluid volume, better volume expansion effect
The domestic consensus points out that the ideal fluid therapy should replenish blood volume effectively and quickly, without increasing the interstitial edema caused by fluid in the extravascular space, without allergies and renal function damage, and without Affect blood coagulation function [5].
Albumin is the main determinant of plasma colloid osmotic pressure and an important part of the acid-base buffer system. The clinical application of human serum albumin is mainly in three concentrations: 5%, 20% and 25%. Research data confirm that the volume expansion effect of 4%~5% albumin is approximately equal to the infusion volume, while the infusion of 20%~25% albumin has three concentrations. Protein can achieve a volume expansion effect that is 4 to 5 times higher than the volume of the infusion solution [5]. Therefore, the high-efficiency expansion capacity of 20%-25% human albumin can help critically ill patients reduce the amount of fluid replacement and avoid the occurrence of fluid overload [6].
my country’s expert consensus suggests that for critically ill patients who need a lot of fluid resuscitation, especially when complicated with acute lung injury, it is recommended to choose albumin for restrictive fluid therapy [5].
Safety and better physiological effects
A study to assess resuscitation fluid requirements and physiologic and clinical responses in ICU patients following volume resuscitation with 20% albumin versus 4% to 5% albumin included the United Kingdom and 321 adult patients in 3 ICUs in Australia requiring volume resuscitation within 48 hours of admission to the ICU. All patients were randomly assigned to receive fluid resuscitation with 20% albumin (n=153) or 4% to 5% albumin (n=168) [2].
The results showed that the fluid volume of patients in the 20% albumin resuscitation group within 48 hours was significantly lower than that in the 4%-5% albumin resuscitation group (P
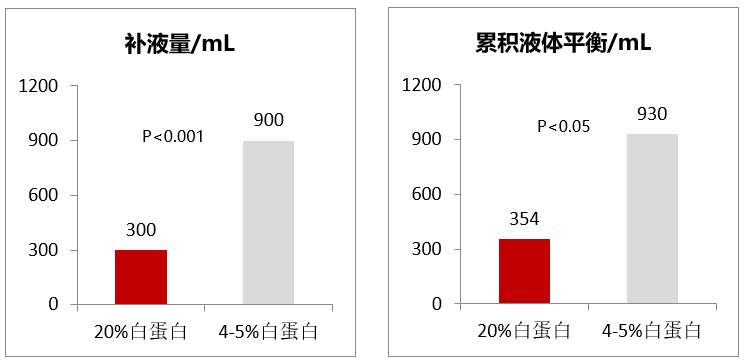
In addition, the 20% serum albumin resuscitation group had higher peak protein levels and lower sodium and chloride levels. The median duration of mechanical ventilation was 12 hours in the 20% albumin group and 15.3 hours in the 4%-5% albumin group; the proportion of patients receiving renal replacement therapy in the 20% and 4%-5% albumin groups was 3.3%, respectively and 4.2% (P=0.67), and the survival rates of patients who were transferred out of the ICU were 97.4% and 91.1% (P=0.02), respectively [2].

Therefore, it is concluded that compared with 4%~5% albumin, the use of 20% albumin for resuscitation can reduce the demand for resuscitation fluid in critically ill patients, and reduce the early fluid positive rate as much as possible. Equilibrium occurs [2].
Summary
Human albumin, as a natural colloid, has the effect of efficient volume expansion, and is a unique choice for rehydration for critically ill patients. Among them, 20%~25% of human albumin has a better volume expansion effect, which can achieve a volume expansion effect that is 4 to 5 times higher than that of the infusion solution. In clinical practice, the type of fluid and treatment plan should be individually selected according to various factors such as the different purposes of fluid therapy, the type of disease, functional hemodynamic state, and the stage of disease development [5].
References:
[1] Chelazzi C, et al (2015) Glycocalyx and sepsis-induced alterations in vascular permeability. Crit Care 19:26.
[2] Mårtensson J, et al. Small volume resuscitation with 20% albumin in intensive care: physiological effects : The SWIPE randomised clinical trial. Intensive Care Med. 2018 Nov;44(11) :1797-1806.
[3] Finfer S, et al (2004) A comparison of albumin and saline for fuid resuscitation in the intensive care unit. N Engl J Med 350:2247–2256.
[4] Caironi P, et al (2014) Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med 370:1412–1421.
[5] Zhao Yupei, Yang Yinmo, Lou Wenhui, Sun Bei, Yu Wenkui. Expert consensus on perioperative fluid therapy for surgical patients (2015) [J]. Chinese Journal of Practical Surgery, 2015, 35 (09):960-966.
[6] PLA Medical Journal, 2012, 37(10):926-929.
Approval Number: VV-MEDMAT-75192
Approval date: September 2022
This information is intended to help healthcare professionals better understand the latest developments in related disease areas. The content of the information published on this platform does not mean that we agree with its description and opinions, but only provides more information. If copyright issues are involved, please contact us, and we will deal with it as soon as possible.
The information provided in this information is not intended to replace professional medical advice in any way and should not be considered medical advice. If such information is used for purposes other than information understanding, this platform, the author and Takeda shall not be held responsible.