The author of this article: Glittering briquettes
“Analgesics should not be used when acute abdomen is not clearly diagnosed, so as not to cover up the disease.” It was once indisputable common sense.
However, in the latest 2019 edition of Internal Medicine, a new chapter on “abdominal pain” was added, which subverted the statement that “there is no evidence that the use of analgesics will Mask abdominal signs or cause increased mortality and disability”, and advocate direct use of morphine:
Internal Medicine advocates giving morphine in undiagnosed acute abdomen
“Our hospital’s emergency room and gastroenterology department use analgesics very actively, but surgery generally insists that acute abdomen is not analgesic.” Dr. Zhang Hao (pseudonym) from a hospital in South China “Maybe they’re still afraid to cover up the disease,” he said.
The textbook “Surgery” published in the same year wrote: “When the diagnosis is not yet clear, strong analgesics are contraindicated, so as not to obscure the development of the disease and delay the diagnosis.”The authoritative “Huang Jia Si Surgery” has a tougher attitude, and it is not recommended to use any type of analgesics.
Surgery presents the exact opposite view
Faced with conflicting textbooks, how does a doctor decide?
Expert consensus that subverts cognition: Analgesics do not delay illness
As early as 1979, it was suggested that in patients with undiagnosed acute abdomen, the early and correct use of analgesics can help the diagnosis while reducing pain [1]. In the decades that followed, this view gained increasing support:
In 1992, a study in the BMJ divided 100 patients with acute abdomen who had just entered the emergency room into two groups. 8.3 in the control group dropped to 3.1 in the experimental group. At the same time, analgesics also improved the accuracy of diagnosis and treatment – compared with 9 people in the control group who were misdiagnosed and mistreated, there were only 2 cases in the experimental group [2].
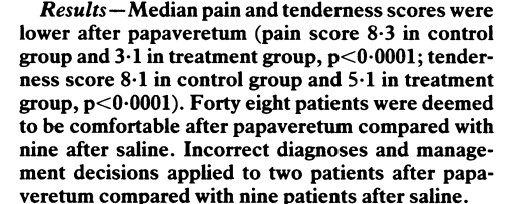
Analgesics may even improve diagnostic accuracy while reducing pain Source: Reference 2
A multi-document pooled analysis yielded similar conclusions. A study in JAMA in 2006 analyzed a large body of literature and concluded that analgesics do not change symptoms and signs, nor do they increase the probability of diagnosis and treatment errors [3]. A 2011 Cochrane database meta-analysis indicated that early use of opioid analgesics did not increase the risk of misdiagnosis [4].
Finally, the American College of Emergency Medicine recommended that patients with acute abdomen be given analgesics after initial evaluation [5]. In Japan, multiple societies jointly launched the “Practice Guidelines for Primary Treatment of Acute Abdomen” in 2015, emphasizing that regardless of the cause of abdominal pain, early analgesia is recommended before the diagnosis is confirmed [6].
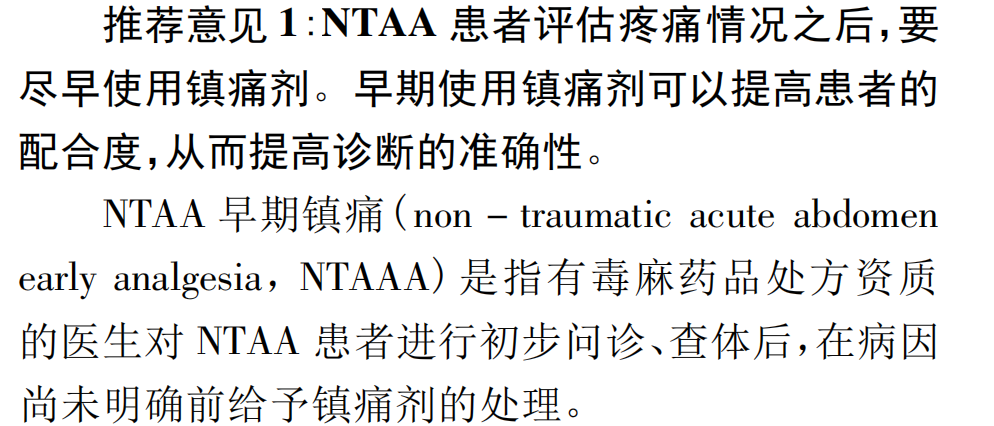
In my country, in 2021, the Department of Emergency Medicine of Peking University released the “Expert Consensus on Early Analgesia for Adult Non-traumatic Acute Abdomen”, which will “NTAA (Non-traumatic Acute Abdomen) ) patients should use analgesics as soon as possible after assessing their pain status. Early use of analgesics can improve the patient’s cooperation, thereby improving the accuracy of diagnosis” as the first recommendation[7].
The
consensus also proposed the concept of early NTAA analgesia, that is, “a doctor with prescribing qualifications for poisonous and narcotic drugs conducts initial consultation and physical examination of NTAA patients, and then administers it before the cause is not yet clear. Analgesics”[7].
Guidance in Expert Consensus on Early Analgesia for Nontraumatic Acute Abdomen in Adults Source: Reference 7
Dr. Liu Si from the Emergency Department of Peking University First Hospital, author of the Expert Consensus on Early Analgesia for Nontraumatic Acute Abdominal Disease in Adults, explains: “Analgesics reduce pain. , but usually doesn’t make the pain go away completely. So it doesn’t mask the condition, especially the important signs.”
“Additionally, analgesics can help doctors make a quick and accurate diagnosis without distractions—for example, a patient with appendicitis who complained of ‘pain all over the abdomen’ could be accurately diagnosed with analgesics It was found that the pain point was actually concentrated in the lower right abdominal pain.”
“At the same time, the doctor-patient relationship will also ease after the use of analgesics.” Dr. Liu Si said, “Many times patients’ biggest request is pain relief, and only after pain relief can they cooperate better. And trust the doctor. If the patient’s pain is left alone, it is not only inhumane, but may also intensify the doctor-patient conflict.” The study also found that doctors tend to underestimate the degree of pain in patients, and this bias will reduce patients’ trust in doctors [ 8].
Over 40 years of opinion, over 50% of doctors disagree
“The severity of the condition may be masked after taking the medicine, and it may also interfere with the judgment of the change of the condition.” Zhang Cheng (pseudonym), the attending physician of a tertiary hospital in North China, does not support this idea.
In a study of emergency physicians at 53 hospitals, 53.8% ofPhysicians disagree with the use of analgesics in patients with undiagnosed acute abdomen, with 97.9% of them citing “fear of weakening signs and affecting diagnosis” as a reason for refusal[9].
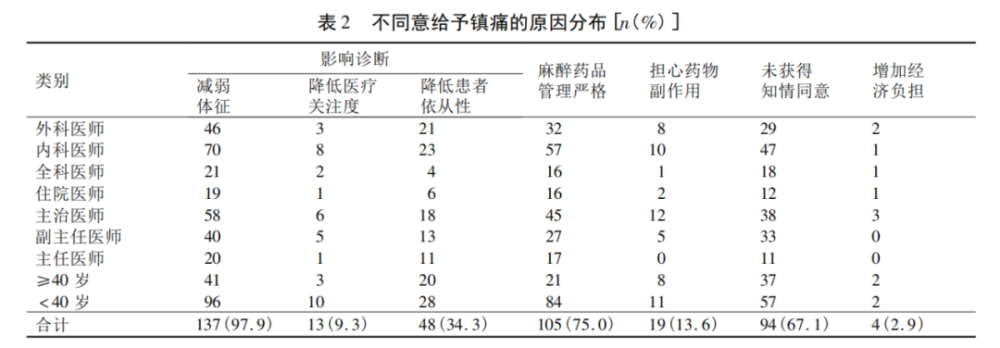
“Reduce signs and affect diagnosis” is the main reason why doctors disagree with analgesia Source: Reference 9
When asked why they couldn’t accept new ideas, many doctors said they had never heard of such a concept.
“Is there still such a thing? We haven’t heard of it.” Wang Qing (pseudonym), a young doctor from a tertiary hospital in East China, said that his hospital did not teach young doctors about this when he taught them. The concept of education, “the teacher did not talk about this expert consensus in class, and we have no way of knowing it.”
Dr. Wang Jinbai (pseudonym) from a hospital in East China reluctantly said: “In fact, many new evidence-based concepts have not been advanced so fast in the hospital.”
Some doctors on the Lilac Garden Forum expressed concern that even if they knew the idea, it was difficult to agree that it was correct. For example, undiagnosed opioid use in patients with pancreatitis may exacerbate the condition by causing the sphincter of Oddi to contract. In addition, opioids are addictive, and non-steroidal drugs are prone to gastrointestinal reactions, which also makes it difficult for doctors to accept such a concept.
When asked why his hospital was able to popularize such a concept, Dr. Liu Si said, “On the one hand, we conduct training based on evidence-based medicine. Tell the doctors how to evolve; at the same time, formulate and implement the medical process, so that doctors can rely on it.”
Careful analgesia, actually used by less than 25% of physicians
Although 46.2% of emergency physicians do not explicitly oppose the use of analgesics, only 24.2% of physicians actually administer analgesia to patients with undiagnosed acute abdomen [9] .
Even accepting the notion that analgesics can be used, physicians tend to be cautious about their use.
Zhang Xuan (pseudonym), the attending physician of a tertiary hospital in East China, said: “In principle, I am not inclined to use analgesics. I use antispasmodics when the pain is severe, but strong Opioids are not used.”
Research also shows that the first choice of doctors is often weak analgesic drugs such as “anisodamine” and “acetaminophen” [9].
Anesthesia drug management is one of the things that hold physicians back. Because hospital management is concerned that if undiagnosed patients can be prescribed analgesics, it will lead to the abuse of analgesics.
“My hospital does not restrict the rational use of analgesic drugs, but has strict procedures in management.” Dr. Liu Si explained, “Doctors can carry out treatment according to the condition. Medication, but the process is stricter than ordinary drugs – such as drug registration, special prescriptions for special colors, etc. This will not hinder the necessary use of analgesics, but also allow doctors to use them carefully.”
“But in addition, we are concerned that patients who use analgesics think that they are cured and no longer cooperate with the treatment. This is a situation that may be encountered in clinical practice. Dr. Liu Si said that if analgesics are used without adequate communication, the patient refuses to take further treatment after the abdominal pain is relieved, which will bring risks to doctors and patients. Explain and communicate well.”
Other doctors pointed out: Perhaps in the “ideal state” of expert consensus, the use of analgesics will not increase misdiagnosis and delay the disease, but the actual clinical and theoretical differences far.
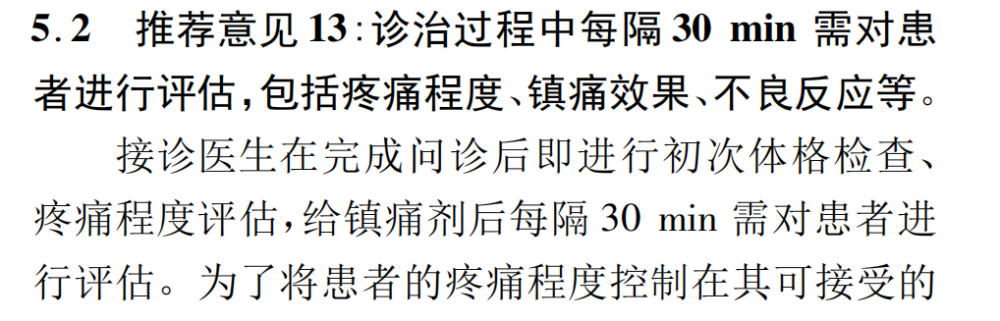
“Expert Consensus on Early Analgesia for Nontraumatic Acute Abdomen in Adults” pointed out that the monitoring of patients should not be relaxed after the use of analgesics, and patients should be evaluated every 30 minutes to avoid misdiagnosis .
However, the emergency departments of some hospitals are so crowded that it is difficult to establish a complete patrol system. Most of the emergency departments and even outpatient clinics do not have a working mode of long-term observation of patients in the hospital, and they prefer to be admitted or discharged after the diagnosis is confirmed, rather than long-term observation of the condition after using analgesics.
“Reduce signs and affect diagnosis” is the main reason why doctors disagree with analgesia Source: Reference 7
“So, such a concept and expert consensus is just a basic handling principle.” Dr. Liu Si said, “How to implement it in specific medical institutions, specific doctors and patients must be implemented. It also needs to be adjusted and refined according to local conditions.”
Conflicting textbooks, how to decide medical disputes?
In addition to whether or not to use analgesics, doctors are more worried about whether there is a medical dispute after use, can someone “support” them? As a medical concept that has just been introduced in China, does a doctor who has the courage to take the lead in applying it have to take greater risks?
According to the China Judgment Document Network, in 2020, a child in Guizhou Province deteriorated and died after surgery, and the family took the hospital to court. The medical appraisal believed that the doctor’s use of strong analgesics violated the principle of “when the diagnosis is not yet clear, strong analgesics are prohibited to avoid covering up the development of the disease and delaying the diagnosis”, and it was finally identified as one of the causes of the accident, and the hospital was responsible for 60 More than ten thousand yuan compensation [10].
Acute abdomen was not diagnosed in the judgmentThe treatment principle of the disease is still “banned strong analgesics” Source: Reference 10
“Whether there is any fault in the medical behavior in such cases is generally carried out by the appraisal department entrusted by the court”, said Zhang Yongquan of Grandall Lawyers (Tianjin) Firm, “It is up to the appraisal party to judge. There are three levels of medical principles that can be taken into consideration as to whether the doctor’s actions violate the medical principles.”
“Textbooks are adopted first, followed by academic monographs, clinical guidelines, drug inserts, etc., and finally, relevant expert consensus can be considered. If there is any conflict, the higher-level opinions will be adopted first. “
The expert consensus in 2021, although this medical concept was officially put forward in China, the priority is lower, and the most convincing is still the textbook. Therefore, in the above precedents, the discussion of “prohibition of potent analgesics” comes from the textbook “Surgery”.
The problem, however, is that the equally authoritative “Internal Medicine” textbook presents completely contradictory views. If there is a dispute, which textbook shall prevail?
“If the textbook views are inconsistent,” lawyer Zhang Yongquan explained, “at this time, an appraiser needs to analyze and judge the relationship between the use of analgesics and the final adverse consequences of the patient according to the submitted materials. Whether there is a direct causal relationship between them.”
“So doctors need to make a clear judgment before giving patients analgesics: Will pain relief affect the judgment of the condition and the treatment plan to be taken?Only the medicine at hand Evidence—such as imaging evidence, laboratory test results, etc.—has already allowed doctors to roughly infer the patient’s condition and rule out serious diseases that require urgent treatment, so that they can stand up to the identification process. “Lawyer Zhang Yongquan gave the doctors such advice.
“In our communication with other doctors, we found that there are indeed concerns about legal disputes.” Dr. Liu Si said, “The expert consensus we launched, on the one hand, wanted to reverse the traditional perception. On the other hand, I also hope to promote the revision and progress of textbooks, so that this evidence-based concept will be unified in the future, so that doctors will no longer have legal risks.”
Acknowledgments: This article has been approved by Liu Si, Deputy Chief Physician and Deputy Chief Physician of the Emergency Department of Peking University First Hospital, and Zhang Yongquan, a lawyer of Grandall Lawyers (Tianjin) Firm. Review
Planning: sparkling briquettes, carollero
Producer: gyouza
Image source: Visual China
References:
[1]Fraser ID. Analgesia and the acute abdomen. Br Med J. 1979 Nov 24;2(6201):1363. doi: 10.1136/bmj.2.6201.1363-b. PMID : 519444; PMCID: PMC1597354.
[2]Attard AR, Corlett MJ, Kidner NJ, Leslie AP, Fraser IA. Safety of early pain relief for acute abdominal pain. BMJ. 1992 Sep 5;305(6853):554 -6. doi: 10.1136/bmj.305.6853.554. PMID: 1393034; PMCID: PMC1883284.
[3]Ranji SR, Goldman LE, Simel DL, Shojania KG. Do opiates affect the clinical evaluation of patients with acute abdominal pain? JAMA. 2006 Oct 11;296(14):1764 -74. doi: 10.1001/jama.296.14.1764. PMID: 17032990.
[4]Manterola C, Vial M, Moraga J, Astudillo P. Analgesia in patients with acute abdominal pain. Cochrane Database Syst Rev. 2011 Jan 19;(1):CD005660. doi: 10.1002/14651858.CD005660.pub3. PMID: 21249672.
[5]Clinical policy: critical issues for the initial evaluation and management of patients presenting with a chief complaint of nontraumatic acute abdominal pain. Ann Emerg Med. 2000 Oct;36(4):406 -15. doi: 10.1067/mem.2000.109446. PMID: 11020699.
[6]https:https://www.sohu.com/a/406945243_377342
[7] Ma Yixiang, Liu Si. Expert consensus on early analgesia for non-traumatic acute abdomen in adults [J]. China Emergency Medicine, 2021, 41(01): 11-17.
p>
[8]Marinsek M, Kovacic D, Versnik D, Parasuh M, Golez S, Podbregar M. Analgesic treatment and predictors of satisfaction with analgesia in patients with acute undifferentiated abdominal pain. Eur J Pain . 2007 Oct;11(7):773-8. doi: 10.1016/j.ejpain.2006.12.002. Epub 2007 Jan 23. PMID: 17251043.
[9] Luo Yi, Li Jiangtao, Fang Hong. Questionnaire survey of emergency physicians on analgesia in patients with unexplained abdominal pain[J]. Southwest National Defense Medicine, 2013, 23(09): 1043 -1045.
[10]https:https://wenshu.court.gov.cn/website/wenshu/181107ANFZ0BXSK4/index.html?docId=93f144001d5e481a812cac08016aafef
Lilac Garden is a professional platform for medical practitioners, with the mission of “helping Chinese doctors”. Download the “Lilac Garden App” to discuss cases with peers, study open classes online, use clinical decision-making tools such as medication assistants, and find reliable medical positions in Lilac Talents.