She was 35 years old. She was diagnosed with “uterine fibroids” because of anemia due to prolonged menstrual period and increased menstrual volume. At that time, her hemoglobin was only 8g/dl, and there was an indication for surgery.
She has had three myomectomy procedures before this.
The patient also wants to preserve the uterus to preserve fertility.
On October 4, 2022, Professor Zhang performed her fourth myomectomy.
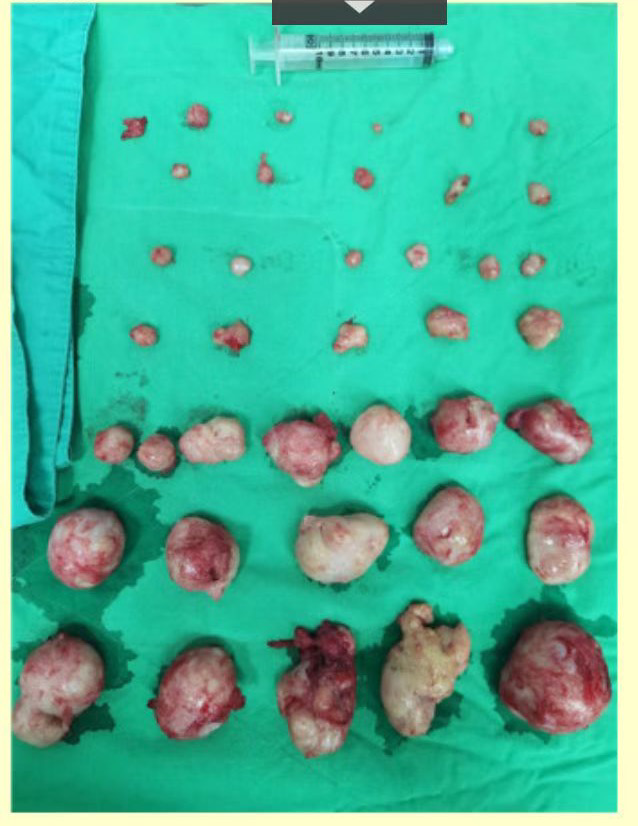
Uterine fibroids removed during surgery.
This surgery is difficult.
On the one hand, she has undergone myomectomy three times, and the entire uterus is scarred, weak, and bleeds easily when the fibroids are removed.
On the other hand, she has an extremely large number of uterine fibroids, as many as 39.
Fortunately, the operation went well and the patient recovered smoothly. It is expected that he will be discharged on the fourth day after the operation.
On October 7, 2022, the third day after the operation, the pathology department sent a pathology report.
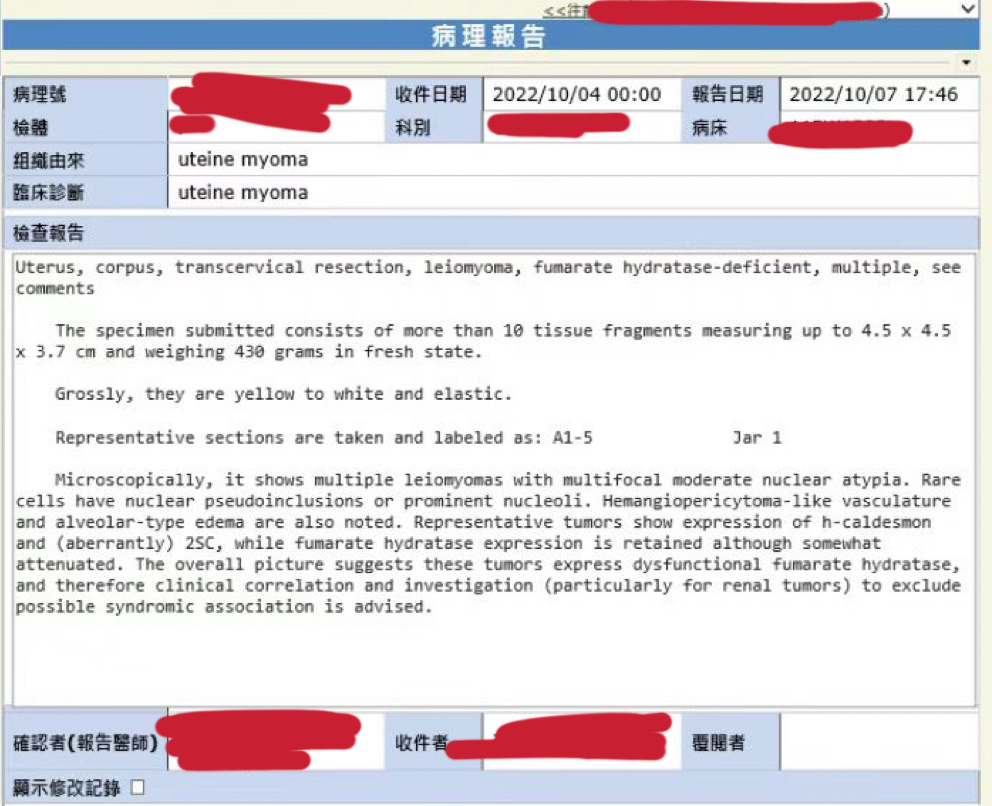
The patient’s pathology report
The pathologist also specially called Professor Zhang, focusing on the discovery of fumarate hydratase deficiency in the specimen (also translated as fumarate hydratase deficiency)
Physicians, in conjunction with the patient’s father, had passed away from kidney cancer, therefore suspecting that the patient was associated with hereditary leiomyomatosis and renal cell carcinoma (HLRCC) Uterine leiomyomatosis.
Professor Zhang immediately instructed the patient to visit the outpatient clinic regularly for follow-up and re-examination. Patients are instructed to pay special attention to regular screening for kidney cancer.
So, what are leiomyomatosis and renal cancer syndrome?
Many young doctors have never heard of this disease!
Because this is a disease that has only been recognized by the medical community in the last ten years and has not been included in textbooks!
Leiomyomatosis and renal cancer syndrome (HLRCC)-related uterine leiomyomatosis is a new disease proposed in the 4th edition of the WHO Classification of Tumors of the Female Reproductive System.
HLRCC-associated renal cell carcinoma was added as an independent disease in the 2016 edition of the WHO Classification of Tumors of the Urological System and Male Genital Organs.
The disease is caused by germline mutation of FH gene, one of the key enzymes of the tricarboxylic acid cycle.
FH gene mutations may interfere with the action of the enzyme in the Krebs cycle, resulting in the accumulation of fumarate.
Researchers believe that excess fumarate may interfere with the regulation of oxygen levels in cells. Chronic hypoxia (hypoxia) in cells with two mutated copies of the FH gene may promote tumor formation and lead to a predisposition to develop leiomyoma and renal cell carcinoma.
Patients developed three main types of tumors: uterine leiomyomatosis, cutaneous leiomyomatosis, and kidney cancer.

1. HLRCC-related uterine leiomyomatosis:
The tumor has a high penetrance rate, ranging from 76% to 100%; the onset is early, and the average age of onset is 30 years old.
Patients have severe symptoms, and about 50% of them undergo myomectomy or even total hysterectomy before the age of 30.
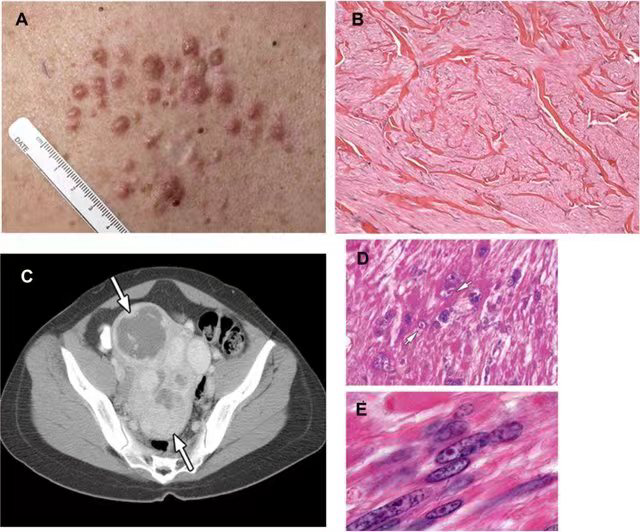
2. HLRCC-related cutaneous leiomyomatosis:
The average age of onset in patients with this tumor is 25 years old, and it is characterized by tan patches or nodules that tend to occur on the extremities or trunk, and its biological behavior is benign.

HLRCC-Associated Cutaneous Leiomyomatosis 1
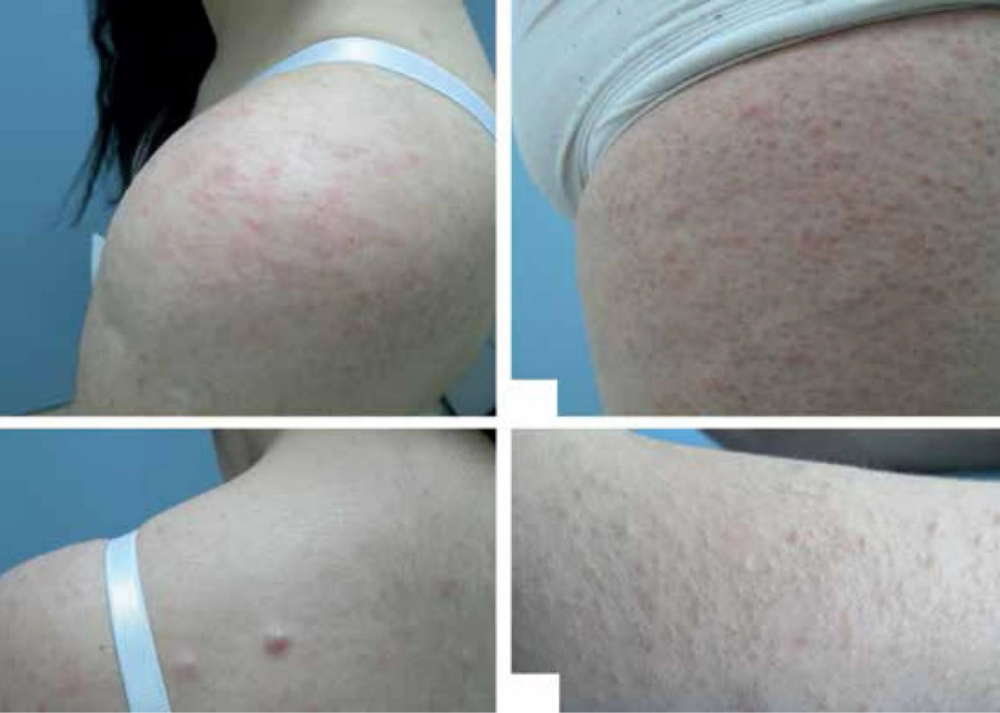
HLRCC-Associated Cutaneous Leiomyomatosis Patient 2
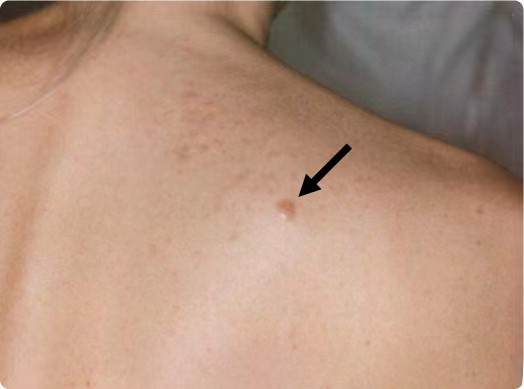
HLRCC-Associated Cutaneous Leiomyomatosis 3

HLRCC-Associated Cutaneous Leiomyomatosis 4
Because sporadic cutaneous leiomyomatosis is extremely rare, once the diagnosis of cutaneous leiomyomatosis is confirmed by pathology, it is highly suggestive of HLRCC.
3. HLRCC-related renal cancer:
This type of renal cancer is mainly type II papillary renal cell carcinoma, and the tumor cell morphology is similar to that of uterine leiomyoma.
Although the penetrance of this tumor is only 15%, its biological behavior is highly aggressive.
Because this type of kidney cancer is often solitary, it is the best treatment plan if it can be detected before the tumor metastasizes and operated in time.
Radical nephrectomy is the first choice for early-stage FH-deficient renal cancer.
But for very early stage tumors or bilateral kidney tumors, wide margin kidney-sparing surgery can also be considered.
Systemic therapy is recommended for advanced FH-deficient kidney cancer.
The treatment plan includes the combination therapy of bevacizumab + Tarceva or target immunity recommended by NCCN guidelines. Through retrospective analysis, TKI monotherapy or PD1 monotherapy is not effective, but target immune combination therapy can also achieve relatively good therapeutic effects.
Since the average age of onset of this type of kidney cancer is 40-46 years old, it is significantly later than uterine and skin leiomyomatosis. Therefore, after the discovery of any tumor in the uterus or skin and the diagnosis of HLRCC , that is, kidney cancer screening should be performed annually.
This is also the meaning of ordinary people who read this article.
Given that 7% of patients develop kidney cancer before the age of 20, patients with a clear family history and a germline mutation of the FH gene can be diagnosed with kidney cancer from the age of 8 to 10 years. Screening.
Uterine smooth muscle tumors are the most common gynecologic tumors.
Patients with uterine fibroids who have one of the following manifestations are recommended to do related genetic testing:
1. The age of onset is earlier than 30 years old, and it recurs after surgical resection.
2. A history of kidney cancer in immediate family members.
3. Nodules appeared on the skin, and the pathological diagnosis was leiomyoma.
At present, many genetic testing companies in China have carried out this genetic testing.
If the patient’s medical history, clinical manifestations and pathological morphology can be combined, the suspected HLRCC-related uterine leiomyomatosis can be screened out and the FH gene germline mutation detection can be carried out, which can promote the early detection of the patient and his relatives. Genetic counseling and kidney cancer screening.
In this way, early detection and early treatment of renal cancer in this type of patients can be achieved, and good curative effects can be achieved.