Writing | Zhou Yebin
With advances in treatment over the past few decades, the 5-year survival rate for childhood cancer has exceeded 80%. But many treatment options also have side effects, such as a delay in the recovery of a patient’s immune system even after chemotherapy has been completed, putting tumor survivors at a higher risk of infection. A survey of childhood cancer survivors showed that the risk of hospitalization due to infection in this group was still 1.6 to 2.7 times higher than that of healthy people after 5 years of treatment. Infections therefore remain a serious health threat to childhood cancer survivors.
While previous studies have shown that childhood cancer survivors have a higher overall risk of infection, data on specific types of infections are relatively lacking, especially those serious infections that can be avoided by vaccination. Without such data, it is difficult for pediatricians to have effective discussions about infection prevention after treatment with childhood cancer survivors themselves and their parents.
A Population-Based Study of the Long- Paper on Term Risk of Infections Associated With Hospitalization in Childhood Cancer Survivors. The study retrospectively analyzed childhood cancer survivors who lived more than 5 years after diagnosis in Washington State, USA, and found that whether it was 5 to 10 years or more than 10 years after diagnosis, survivors still faced higher rates of hospitalization due to infection risks, including those infections that can be effectively prevented by vaccination. This study not only fills the knowledge gap in this field, but also provides a data basis for more effective communication with patients and their families about the risk of infection after treatment.
Researchers enrolled childhood cancer survivors from two tumor surveillance systems in Washington State, USA. The study entry criteria were childhood cancer patients diagnosed between 1982 and 2008, and the survival time after diagnosis was at least more than 5 years. Ultimately, 3152 childhood tumor survivors met the criteria to make up the study cohort. Among them, 39.5% of the patients were hematological tumors, and 60.5% of the patients were non-hematological tumors. The most common tumors were leukemia (25.9%), central nervous system tumors (19.8%) and lymphoma (13.6%). The median age at tumor diagnosis among survivors was 7 years, and the median follow-up time was 8.8 years from 5 years after diagnosis. 48.1% of survivors were female and 51.9% were male. The researchers also randomly matched each survivor to 10 controls of the same age and sex using Washington state birth records to create a comparative cohort of healthy people.
During the follow-up period, 382 hospitalizations for infection occurred among 3152 childhood tumor survivors; 771 hospitalizations for infection occurred among 31519 healthy controls. This means that among tumor survivors, the incidence rate (IR) of infection hospitalization was 12.6 per 1000 person/year; the IR of healthy controls was 2.4 infection hospitalization per 1000 person/year. The incidence of hospitalization for infection (IR) for hematoma and non-hematoma survivors was 18.5 and 8.7, respectively. Bacterial infection was the most common type of infection in both types of survivors, with IRs of 7.3 and 2.7, respectively. In terms of infection site, respiratory tract infections were the most common in hematoma survivors, with an IR of 4.1, and non-hematoma survivors had similar rates of respiratory infections and genitourinary infections.
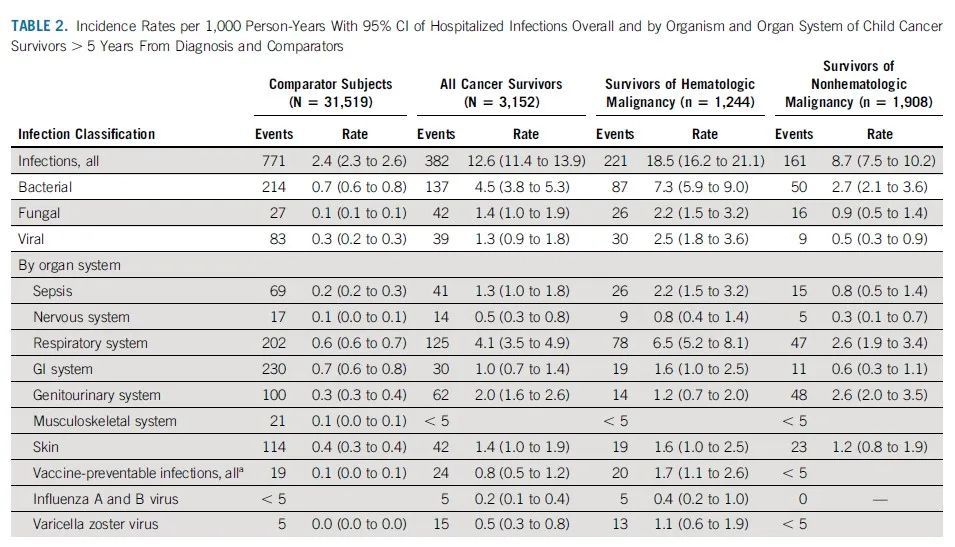
Overall incidence of hospitalized infection and incidence by infection type and organ in survivors and healthy controls
It is important to note thatinfection rates decreased over time in both hematologic and non-hematologic survivors. 5-10 years after diagnosis, the infection incidence rate (IR) for survivors was as high as 18.1, and 10 years later it dropped to 8.3. However, this was still significantly higher than the incidence of infection in healthy controls during the same period (2.5 and 2.6, respectively).

Comparison of the incidence of infection 5-10 years after diagnosis and 10 years later (A all types of infections, B bacterial infections, C fungal infections, D viral infections)
The incidence rate shows the overall risk rate of infection and hospitalization. In addition to this, attention should be paid to whether the relatively healthy population, childhood cancer survivors, have a higher risk of infection, that is, the relative incidence rate (incidence rate ratio, IRR). The overall IRR for all childhood cancer survivors in the study was 5.1. Although bacterial infections are quantitatively the most common type of infection in both hematoma and non-hematoma survivors. But the relative risk was higher for fungal infections, with an IRR of 25.2 for hematoma survivors and 10.2 for non-hematoma survivors. In terms of infected organs, the highest relative risk for hematoma survivors was the nervous system, with an IRR of 13.9, followed by the respiratory tract, with an IRR of 10.1. The highest relative risk in non-hematoma survivors was the genitourinary system with an IRR of 8.1, followed by the nervous system with an IRR of 5.0.
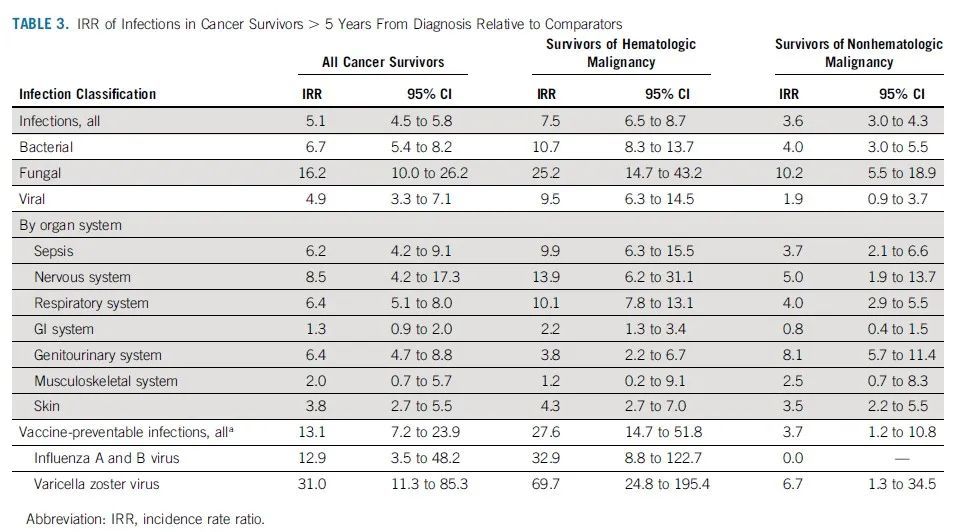
Infection Risk (IRR) in Cancer Survivors Relative to Healthy Controls
Vaccination-preventable hospital infection rates are low in both childhood cancer survivors and healthy controls. However, the specific incidence was still higher in cancer survivors than in healthy controls (IRR 13.1). In particular, both hematoma and non-hematoma survivors had a high risk of varicella-zoster virus infection (IRR 69.7 and 6.7 in both groups, respectively). Because the vast majority of survivors in the study were born at a time when the varicella vaccine was not part of the childhood vaccination program in the United States, it was not possible to determine whether the higher risk of hospitalization for varicella-zoster infection was due to vaccine failure. Hematoma survivors also have a higher risk of hospitalization for influenza virus infection.
Complete the full text,This study shows childhood cancer survivors have a higher risk of being hospitalized for infection. Although the risk of infection 10 years after diagnosis was lower than that between 5 and 10 years after diagnosis, even 10 years after diagnosis, childhood cancer survivors had a significantly higher risk of hospitalization for infection than healthy controls. In addition, although hematoma survivors have a higher risk of infection, the risks faced by non-hematoma survivors cannot be ignored, regardless of the type of infection and the infection of which organ system, the risk faced by non-hematoma survivors still higher than that of the general healthy population. From these results, physicians of childhood cancer survivors need to communicate long-term infection risks after treatment to survivors and families. In the event of an infection, more aggressive interventions, such as direct hospital visits, may also be required.
In addition, childhood cancer survivors are at higher risk even for infections that are preventable by vaccination. This may require more research in the future to improve the response plan. Like a higher risk of influenza hospitalization that may warrant an emphasis on annual influenza vaccination, cancer survivors may also need to make up for missing vaccinations or revaccination after treatment. As the prognosis of childhood cancer continues to improve, prevention of long-term infection risk should also be a key focus area to improve the health burden of childhood cancer survivors.
Writing
Production
Typesetting | Sheila proofreading | uu