Patients often visit an ear doctor because of hearing loss, and a small number of patients are diagnosed with “otosclerosis” after being examined by a specialist. What about otosclerosis? With this question in mind, the author interviewed Li Li, director of the Department of Ear Surgery of Shandong Otolaryngology Hospital.
First of all, we need to understand how we hear sound. A complete sound perception process is more complicated.
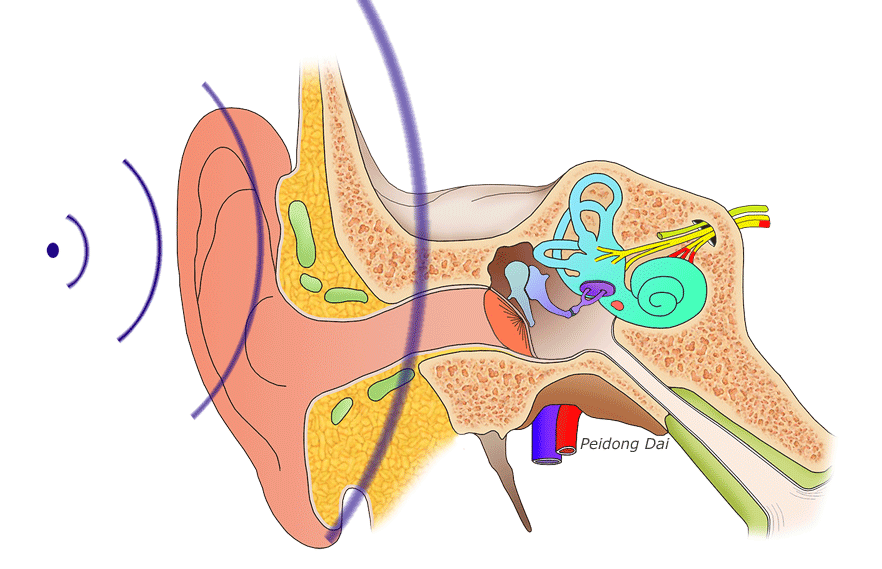
There are many complex structures in the ear responsible for receiving sound, transmitting sound, converting sound signals, and the brain’s perception of sound. First, the auricle transmits the collected sound to the tympanic membrane through the external auditory canal, and causes the tympanic membrane to vibrate, thereby driving the ossicular chain to vibrate together, and then causing the lymphatic fluid of the inner ear to vibrate and stimulate the hair cells to perform acoustic and electrical transduction work. Nerve impulses are transmitted to the brain through the auditory nerve, and finally pass through our brain to sense sound. Problems or failures in any of these links will cause our hearing loss. According to the damage site and the size of the hearing loss, it is called different types and degrees of deafness.
Otosclerosis is a condition in which the movement of the stapes is limited or fixed, resulting in hearing loss. The onset of otosclerosis may be genetically related. The stapes is the smallest bone in our body, about the size of a grain of rice and shaped like a stirrup. Otosclerosis is pathologically manifested as primary localized bone resorption in the bony labyrinth of the inner ear, and replaced by spongy bone hyperplasia with abundant blood vessels. Early lesions only affect the activity of the stapes, resulting in conductive hearing loss. When the lesions are larger and involve the vestibular window and the cochlea at the same time, it is called diffuse otosclerosis, and the semicircular canal, internal auditory canal and facial canal can also be involved, resulting in vertigo and sensorineural hearing loss.
Otosclerosis often presents as progressive hearing loss, often with a family history. More bilateral than unilateral. Some patients may be accompanied by tinnitus, and a few patients may also be accompanied by vertigo. Another feature is that patients with otosclerosis cannot hear clearly in a quiet environment, but in a noisy environment, the patient feels that they can hear clearly, which is called “Wechsler’s mishearing” in medicine. In addition, the tone of speech of patients with otosclerosis is mostly “soft voice”, rather than a high-pitched trumpet-like speech, which is significantly different from the “loud voice” of patients with sensorineural deafness.
Based on the above characteristics, many cases of otosclerosis may be overlooked and underdiagnosed. The tympanic membrane of these patients is basically normal, unlike otitis media with perforated tympanic membrane, doctors usually need to do some examinations, such as high-resolution CT of the temporal bone, etc., to rule out tympanic sclerosis caused by otitis media or congenital ossicular chain deformity.
In the early stage of otosclerosis, surgery or bone conduction hearing aids can be considered for conductive hearing loss, and for moderate or severe sensorineural hearing loss in the later stage, hearing aids or cochlear implant surgery can be used to reconstruct hearing. Generally speaking, most patients with conduction deafness can be greatly improved by surgical treatment, but there is also a risk of neural deafness, which needs to be carefully considered.
Li Li, Director of Ear Surgery, Shandong Otolaryngology Hospital, warmly reminds: When you have hearing loss, tinnitus and other symptoms, you should seek medical attention in time.