The 58-year-old Wang has been struggling with swallowing and coughing from time to time in recent months. So he went to the hospital to find a doctor to see what was going on.

After listening to his description, the doctor analyzed that he may have an esophagus problem. From a professional point of view, patients with early-stage esophageal cancer can mainly present with retrosternal discomfort, burning sensation or pain, and when food passes through, there may be a sense of foreign body or friction locally.
In order to reduce the pain, he also accepted the doctor’s suggestion to do a painless gastroscopy.
On the day of the gastroscopy, I lay on the examination bed with an uneasy mood.
Unexpectedly, he almost never got up again when he lay down.
After seeing several of his tests, the anaesthetist slowly injected the anaesthetic.
After more than ten seconds, he closed his eyes.
Trying his eyelash response, the gastroscopist inserted a gastroscope.
Seeing that the gastroscope was inserted smoothly and Pharaoh didn’t respond, the anesthesiologist felt relieved.

The most critical part of the painless gastroscopy process is the mirror entry stage: on the one hand, the patient is required to be immobile; on the other hand, the patient must be kept breathing smoothly.
Some people say that shallow anesthesia is enough?
No. With shallow anesthesia, not only the patient moves easily, but also adverse reflexes such as arrhythmia or airway spasm occur.
And deep anesthesia may cause respiratory depression. At this point, the gastroscope occupies the airway, often making it difficult for the anesthesiologist to control the airway. Therefore, any anesthesiologist will be nervous at this stage.
Suddenly, the anesthesiologist’s heart lifted up again. The reason is that the patient’s blood oxygen plummets almost straight. In this case, there is a high probability of suffocation.
Under normal circumstances, doctors should investigate the cause step by step. But when this happens, the doctor hardly gives the doctor a chance to think about it, and will directly think about the worst result.
However, curiously, the patient appears to be choking at the same time.
It’s only been a few minutes since the medicine was given, so it’s impossible to metabolize it so quickly. Besides, this is an old man. The anesthesiologist was puzzled.

After confirming that the patient had no airflow through the nose, the anesthesiologist asked the gastroscopist to quickly pull out the gastroscope. Subsequently, the patient was quickly pressurized and controlled to breathe with a simple respirator.
With several strong pressurized oxygen doses, gas moves in and out of the patient’s lungs.
Look at the monitor again, and the blood oxygen, which is almost at the end, begins to pick up.
Seeing the patient out of danger, the anesthesiologist is there to think: What caused this? After working for so many years, this is the first time I have encountered such severe respiratory depression.
During the analysis, a large puddle of water suddenly came out from the corner of the patient’s mouth.
Suddenly, the anesthesiologist thought that it might be caused by the gastroscopist giving water in the esophagus.

When he turned to look at the gastroscopist, he hurriedly explained that all the water he was given was sucked out. The water is in front of the lens, and the suction hole is in the proximal esophagus, so it is impossible to have so much water in the esophagus.
Speaking in a tone that is obviously trying to clear the relationship.
Looking back at the patient’s vital signs, there was no major problem, and the anesthesiologist didn’t pursue it any further.
Although there were some problems, since the patients were all anesthetized, the patients could not be allowed to spend money in vain, so everyone agreed to continue this gastroscope. If there is abnormality, give up the gastroscopy.
This time, the gastroscopist did not dare to use any water.
As I was walking, a hole appeared in the lens of the gastroscope, a hole that seemed to have gas going in and out.
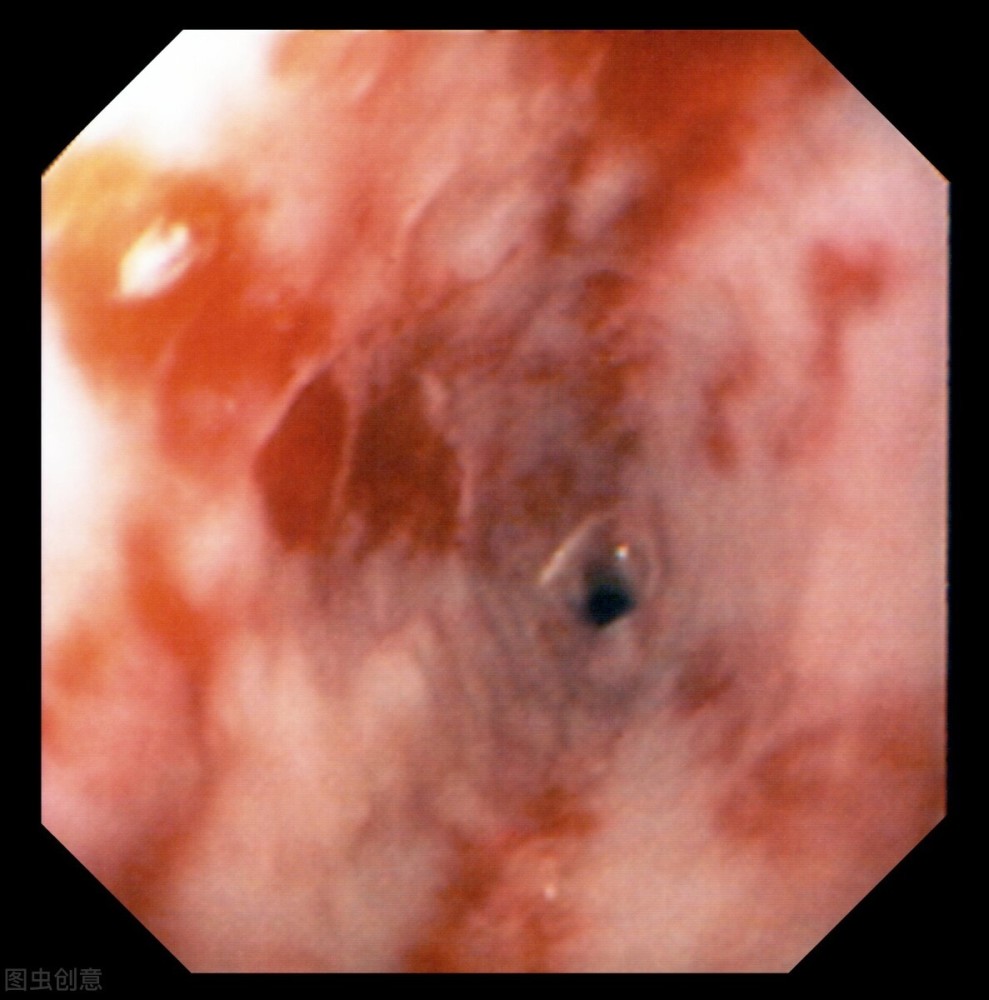
I have been in contact with various tumors all day, and everyone immediately thought of esophagotracheal fistula. Yes, this is the disease!
As soon as this result appears, it can fully explain the previous suffocation. It is because of the existence of this hole that the water normally given by the gastroscopist accidentally enters the trachea and causes suffocation.
At the same time as the cause was identified, it also taught everyone a profound lesson: when you know that the patient may have esophageal cancer, you should think more about whether there is a problem that may involve the airway. .
[Warm reminder] Please pay attention, here are a lot of professional medical science, to reveal the secrets of surgical anesthesia for you~