A few days ago, a patient came to the outpatient clinic and asked a very popular question. He said, the surgeon told me that my operation was successful and the tumor was cut cleanly. Who is the surgeon? How can you tell if the cut is clean? Now that the cut is clean, does it mean that there will be no recurrence?
This is a question that many patients are eager to know. Generally speaking, after the surgeon removes the tumor on the day of the operation, it will be sent to the family members outside the operating room as soon as possible, and then they will say that the operation was successful and the tumor was cut cleanly. This is actually only a success seen by the naked eye, mainly in accordance with the surgical operation guidelines and clinical experience, the tumor was completely removed, and the corresponding lymph node dissection was performed.

In fact, it is very important to judge whether a lung cancer patient has undergone radical resection, not only including standardized surgical procedures and intraoperative resection with the naked eye, but also more important It is to look at the postoperative pathology. In 2005, the Staging Committee of the International Association for the Study of Lung Cancer proposed the definitions of “complete resection, “incomplete resection” and “indeterminate resection” for lung cancer surgery. Among them, complete resection is R0 resection, which includes the following points:
1. Systematic or lobar-specific lymph node dissection should be performed, and the lymph nodes should include at least 6 groups, including intrapulmonary (lobar, interlobar or segmental) and/or hilar group 3 [N1], Mediastinal group 3 (N2, must include zone 7).
2. Postoperative major pathology, the margins must be negative, including bronchial, arterial, vein, peribronchial, and tissue near the tumor.
3. Postoperative pathology showed that there was no extranodal invasion in the respectively resected mediastinal lymph nodes or marginal lymph nodes of the resected lobe.
4. The highest lymph node resected was negative under microscope.
All the above four points can be said to be true R0 surgery, radical surgery. For 1. positive surgical margins; 2. extranodal invasion of the resected mediastinal lymph nodes or marginal lymph nodes of the resected lobe; 3. the presence of unresectable positive lymph nodes; 4. pleural effusion or pericardial effusion can detect cancer cells ; Any of these four points is incomplete excision. Among them, microscopic residual tumor is R1, and macroscopic residual tumor is R2.
The difference in prognosis between complete and incomplete resection is considerable. For example, a retrospective study in Italy, 1277 patients who underwent lung cancer resection, the 5-year survival rates of complete resection and incomplete resection were 58.8% and 15.7%, respectively. The difference is obvious. Of course, no doctor does not want the operation to be successful. Most of the reasons for patients who fail to complete resection are because the patient’s disease stage is too late and the tumor location is not good. The reasons related to the lack of doctor’s skills and experience are only a few.
With the development of molecular biology, a new detection method has been introduced to judge whether the surgery has achieved true complete resection. This detection method is MRD detection. MRD is an emerging technology that detects the DNA of tumor cells in peripheral blood through next-generation gene sequencing. A positive result means that residual (remaining) lesions can still be detected after surgery, and these residual cancer cells will become active later. and begin to multiply, causing the disease to recur. For MRD-positive lung cancer patients, postoperative adjuvant therapy is generally recommended to reduce the probability of recurrence and metastasis. Gene

How can I know if my lung cancer surgery is clean?
A few days ago, a patient came to the outpatient clinic and asked a very popular question. He said, the surgeon told me that my operation was successful and the tumor was cut cleanly. Who is the surgeon? How can you tell if the cut is clean? Now that the cut is clean, does it mean that there will be no recurrence?
This is a question that many patients are eager to know. Generally speaking, after the surgeon removes the tumor on the day of the operation, it will be sent to the family members outside the operating room as soon as possible, and then they will say that the operation was successful and the tumor was cut cleanly. This is actually only a success seen by the naked eye, mainly in accordance with the surgical operation guidelines and clinical experience, the tumor was completely removed, and the corresponding lymph node dissection was performed.
In fact, it is very important to judge whether a lung cancer patient has undergone radical resection, not only including standardized surgical procedures and intraoperative resection with the naked eye, but also more important It is to look at the postoperative pathology. In 2005, the Staging Committee of the International Association for the Study of Lung Cancer proposed the definitions of “complete resection, “incomplete resection” and “indeterminate resection” for lung cancer surgery. Among them, complete resection is R0 resection, which includes the following points:
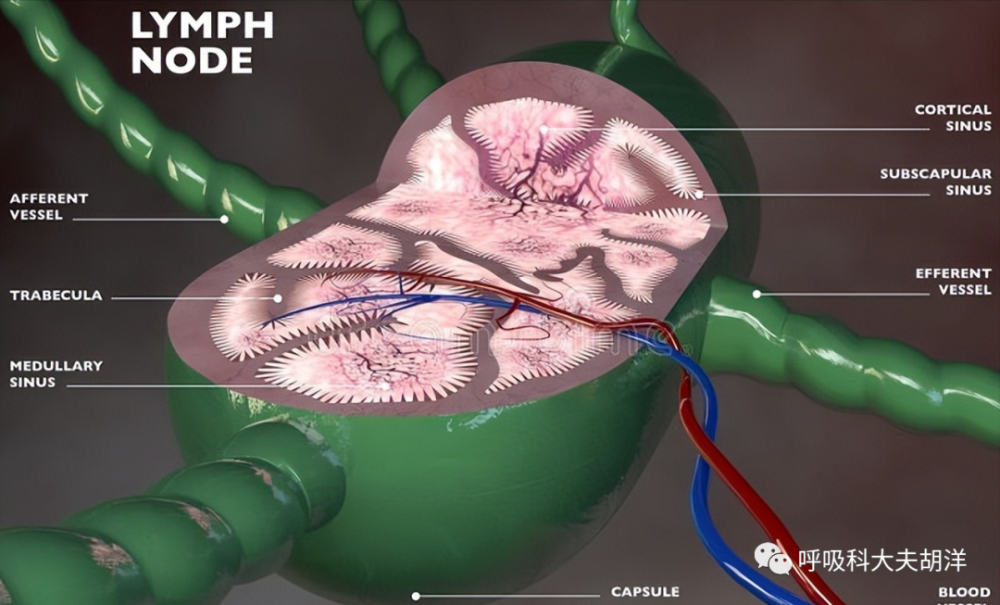
1. Line systemFor sexual or lobar-specific lymph node dissection, the lymph nodes should include at least 6 groups, including intrapulmonary (lobar, interlobar, or segmental) and/or hilar group 3 [N1], and mediastinal group 3 (N2, which must include area 7).
2. Postoperative major pathology, the margins must be negative, including bronchial, arterial, vein, peribronchial, and tissue near the tumor.
3. Postoperative pathology showed that there was no extranodal invasion in the respectively resected mediastinal lymph nodes or marginal lymph nodes of the resected lobe.
4. The highest lymph node resected was negative under microscope.

All the above four points can be said to be true R0 surgery, radical surgery. For 1. positive surgical margins; 2. extranodal invasion of the resected mediastinal lymph nodes or marginal lymph nodes of the resected lobe; 3. the presence of unresectable positive lymph nodes; 4. pleural effusion or pericardial effusion can detect cancer cells ; Any of these four points is incomplete excision. Among them, microscopic residual tumor is R1, and macroscopic residual tumor is R2.
The difference in prognosis between complete and incomplete resection is considerable. For example, a retrospective study in Italy, 1277 patients who underwent lung cancer resection, the 5-year survival rates of complete resection and incomplete resection were 58.8% and 15.7%, respectively. The difference is obvious. Of course, no doctor does not want the operation to be successful. Most of the reasons for patients who fail to complete resection are because the patient’s disease stage is too late and the tumor location is not good. The reasons related to the lack of doctor’s skills and experience are only a few.
With the development of molecular biology, a new detection method has been introduced to judge whether the surgery has achieved true complete resection. This detection method is MRD detection. MRD is an emerging technology that detects the DNA of tumor cells in peripheral blood through next-generation gene sequencing. A positive result means that residual (remaining) lesions can still be detected after surgery, and these residual cancer cells will become active later. and begin to multiply, causing the disease to recur. For MRD-positive lung cancer patients, postoperative adjuvant therapy is generally recommended to reduce the probability of recurrence and metastasis.