*For medical professionals only
Myocardial infarction is not a disease for middle-aged and elderly people!
With the transition of the aging population structure, the accelerated pace of life and the increase of work pressure, coronary heart disease has gradually become a major killer threatening human health, and it is also the most common cause of sudden death among young and middle-aged people. Common causes. Words such as “acute myocardial infarction”, “sudden death” and “overwork” are frequently seen in the newspapers, and the trend of myocardial infarction becoming younger is more and more obvious.
People are increasingly wondering, is there an age cutoff for myocardial infarction? At what age should attention be paid to the prevention of acute myocardial infarction? What if the author told you that newborns also get acute myocardial infarction?

Start with a case!
Suddenly worsened 2 hours after birth
A 36-week gestational mother who underwent a cesarean section for placenta previa has experienced pregnancy bleeding as early as 35 weeks of gestation. The delivery went smoothly, with an Apgar score of 9 on both occasions. Routine postnatal examination, the baby’s fetal heart unload test was normal, and echocardiography also showed that the heart structure and function were completely normal.
However, just about 2 hours after birth, the baby suddenly developed shortness of breath, respiratory distress, and cyanotic skin.
The results of the physical examination are as follows:
Body temperature 36.6℃, respiratory rate 85 beats/min, blood pressure 58/31mmHg, heart rate 147 beats/min.
Decreased blood oxygen saturation: the upper extremity oxygen saturation was 92%, while the lower extremity oxygen saturation dropped to 78%; blood gas analysis showed metabolic acidosis (pH2.3, HCO3-17mmol /L, BE-10.0 mmol/L, lactate 7.3 mmol/L); bilateral pulmonary edema was seen on chest X-ray; bedside echocardiography showed severely reduced left ventricular systolic function.
All test results suggest that the child’s heart may have serious disease that is progressing rapidly. The patient was then urgently transferred from the neonatal general care unit to the neonatal intensive care unit.
Why does a 2-hour-old newborn suddenly develop cyanosis of different degrees of upper and lower extremities with left ventricular insufficiency?
Differential Diagnosis: Differential Cyanosis
Differential cyanosis (differential cyanosis) is a basic concept in pediatrics. It is more common in children with patent ductus arteriosus, and the blood is continuously shunted from left to right. lead to pulmonary hypertension. When the pulmonary artery pressure exceeds the aorta, the left-to-right shunt is significantly reduced or stopped, resulting in a reverse shunting of the pulmonary artery blood flow into the descending aorta. The lower limbs are heavier than the upper limbs, and the left upper limb is heavier than the right upper limb, that is, differential cyanosis.
However, this patient was only 2 hours old, and it is unlikely that a right-to-left shunt would have developed so soon, even in the presence of a patent ductus arteriosus.
In addition to patent ductus arteriosus, left heart obstructive lesions (eg, aortic arch dysplasia, aortic arch dissection, severe aortic coarctation, and severe aortic valve stenosis) may also cause Differential cyanosis. Differential cyanosis may also occur due to decreased cardiac output, where blood supply to the lower extremities is compensated by a patent ductus arteriosus. Other causes include cardiomyopathy, myocarditis, coronary artery dysplasia, thrombosis, and dissection.
What exactly is the reason for a 2-hour-old newborn?
After being transferred to the intensive care unit, the doctor perfected the relevant examinations for the child, and the results showed that the myocardial markers were significantly increased: troponin 12ng/ml, creatine kinase isoenzyme (CK) -MB) 135.6ng/ml; ECG showed QS type in leads I and aVL (see Figure 1), suggesting left ventricular lateral wall myocardial infarction.
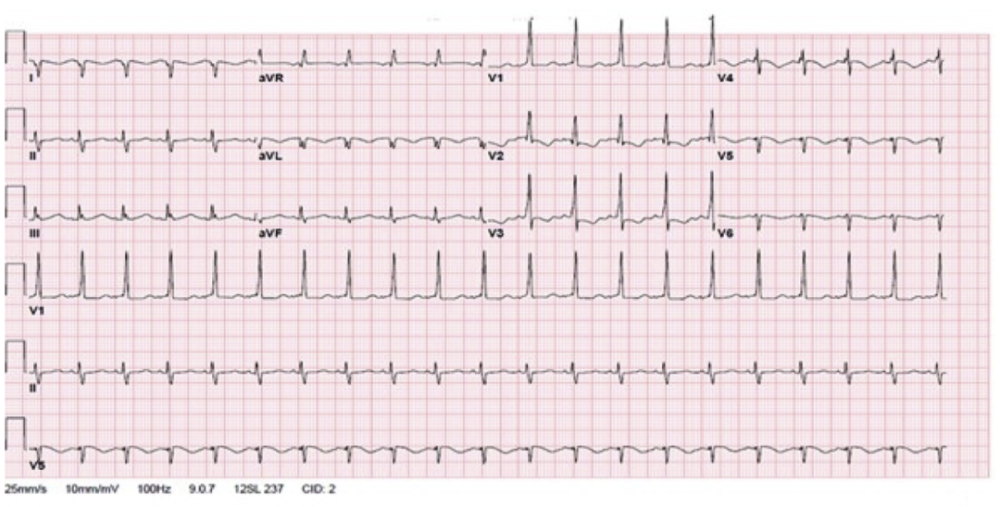
Fig. 1 The ECG of the child shows a QS pattern in leads I and aVL, suggesting left ventricular lateral wall myocardial infarction.
Heart echocardiography showed severely reduced left ventricular function (LVEF 25%), moderate-to-severe mitral regurgitation, and no significant aortic stenosis or coarctation.
The condition of the child continued to deteriorate, and the monitoring indicators continued to rise. The drug treatment effect was not good. In the end, extracorporeal life support—Extracorporeal Membrane Oxygenation (ECMO) was the only option. ).
After the vital signs remained stable, the doctor performed a detailed echocardiography again. The origin of the coronary arteries was completely normal, but atthe aortic root, A hyperechoic band wafting with the blood flow was found near the ostium of the left coronary artery (see Video 1).
Further analysis revealed that the band was membranous and extended to the left main opening. Is it thrombosis or aortic dissection?
Video 1 A strong echogenic band with blood flow can be seen at the opening of the left coronary
Having doubts, the doctor performed an invasive interventional examination for the baby just a few hours after birth. After injecting a contrast agent into the aortic root, it was found that a large number of thrombi were visible in the left main vessel, although no Complete occlusion, but only a small amount of contrast medium can pass through the distal vessels.
The child was then sent to surgery for a thrombectomy. Postoperative pathology confirmed a red thrombus of 0.9cm×0.1cm×0.05cm (see Figure 2).
Figure 2 A thrombus removed from the patient’s left main trunk
After the operation, the patient’s condition gradually stabilized, and various indicators gradually improved. On the 7th day after the operation, the patient was successfully released from ECMO. One month after the operation, the child was discharged from the hospital, and at this time, there was still mild left ventricular systolic insufficiency (LVEF 48%) on repeat echocardiography. After 3 months of re-examination, the cardiac function has returned to normal (LVEF56%).
Why does a newborn baby get a heart attack?
Clinically common coronary heart disease and acute myocardial infarction mostly occur on the pathological basis of coronary atherosclerosis, which is caused by plaque rupture or plaque erosion. A 2-hour-old baby is obviously not likely to develop coronary atherosclerosis, and the coronary artery development is completely normal, but acute myocardial infarction occurs due to thromboembolism. What is the reason?
According to literature reports, high-risk factors for neonatal coronary thrombosis include: hypercoagulable state in vivo, fetal immaturity, neonatal asphyxia, myocarditis, delayed intubation Umbilical, umbilical venous catheter placement, and paradoxical embolism due to right-to-left shunt due to patent ductus arteriosus.
After confirming the thrombosis, the doctor screened the above-mentioned causes one by one. The childbirth process was normal and there were no other risk factors. The blood coagulation-related indicators (PT, APTT, TT, fiber Protein pro, antithrombin III, protein C, protein S and V factor Leiden mutation, etc.) were normal. For the baby in this case, although it is still premature, but the development is mature, and the blood coagulation indicators are normal, the cause of myocardial infarction has become a mystery.
Have you seen a younger MI patient? Or have you heard of similar cases of “senile disease” occurring in infants and young children? What is the reason?
Welcome to leave a message in the comment area~
References:
[1] Neha Ahluwalia, Robert H. Pass, Scott I. Aydin. Newborn With Severely Depressed Left Ventricular Function: Acute Myocardial Infarction in a Newborn. J Am Coll Cardiol Case Rep. 2020; 2(12):1837-1840.
[2] Papneja K, Chan AK, Mondal TK, Paes B. Myocardial Infarction in Neonates: A Review of an Entity with Significant Morbidity and Mortality. Pediatr Cardiol. 2017;38(3) :427-441.
[3] Streif W. Myocardial infarction in a neonate. Lessons for neonatal and internal medicine. Hamostaseologie. 2017;37(3):219-222.
[4]Peeters S, Vandenplas Y, Jochmans K, et al. Myocardial infarction in a neonate with hereditary antithrombin III deficiency. Acta Paediatrica.1993;82:610C3.
[5]Bernstein D, Finkbeiner WE, Soifer S, Teitel D. Perinatal myocardial infarction: a case report and review of the literature. Pediatr Cardiol.1986;6:313C7.
[6]. Poonai N, Kornecki A, Buffo I, Pepelassis D.Neonatal myocardial infarction secondary to umbilical venous catheterization: a case report and review of the literature. Paediatr Child Health.2009; 14:539C41.
This article was first published: Medical Pediatrics Channel
This article was written by Myelin
Editor in charge: Yuan Xueqing, Zhang Li
Copyright Notice