Research background and purpose
Invasive candidiasis is the most common fungal infection in hospitalized patients worldwide and is associated with high mortality and prolonged hospital stay. However, due to the complexity of treating invasive candidiasis (eg, infectious pathogen characteristics, disease severity, patient characteristics), and the different pharmacological effects, costs, and adverse events of related drugs, the optimal treatment regimen with high efficacy and low toxicity is established Still a challenge. A recent study (IF: 15.441) published in the International Journal of Antimicrobial Agents evaluated and compared the efficacy and safety of antifungal drugs in the treatment of candidemia.
Research Methods
Researchers conducted systematic reviews using network meta-analysis (NMA), surface area under cumulative ranking analysis (SUCRA), and randomized multi-criteria acceptability analysis (SMAA). PubMed and Scopus were searched for analyses of randomized controlled trial studies evaluating cure rates, discontinuation rates, and adverse events of oral antifungal drugs (any dose or regimen) for invasive candidiasis.
Study Results
Investigators analyzed a total of 13 trials (n = 3632) and established 5 NMAs for different doses and schedules of antifungals: Overall response to treatment (clinical and microbiological ), microbiological response, disease recurrence, treatment discontinuation due to adverse events and abnormal liver function (most reported adverse events) (Figure 1), and there were no significant differences in efficacy outcomes between treatments. However, caspofungin (50-150 mg), rezafungin (200-400 mg) and micafungin (100-150 mg) had higher clinical and mycological response rates (SUCRA overall response > 60%) (Fig. 2), which has more therapeutic prospects. Fluconazole (400 mg) had the worst overall response (17%). Discontinuation rates were low (<40%) for Rezafungin (200-400 mg) and micafungin (100 mg). Regular amphotericin B (0.6-0.7 mg/kg) is more likely to be discontinued [compared with caspofungin 150 mg, odds ratio (OR) 0.08; 95% confidence interval (Crl) 0.00-0.95] and may harm Liver function (87%).
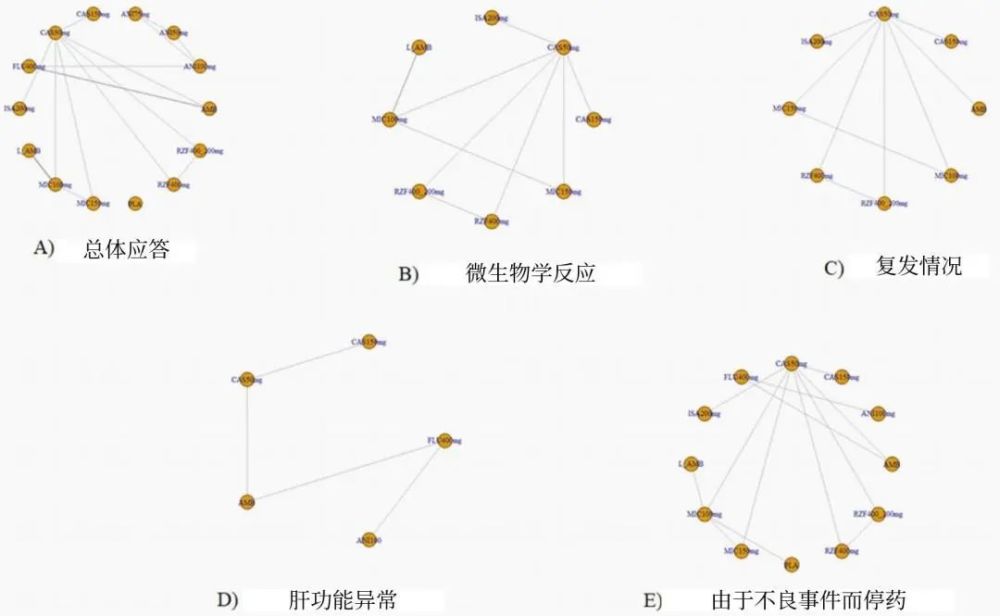
Figure 1 Outcome and treatment comparison network diagram of each trial
Note: Directly comparable interventions are connected by a line whose thickness is proportional to the number of trials per comparison. AMB: conventional amphotericin B; ANI: anidulafungin; CAS: caspofungin; FLU: fluconazole; ISA: isavuconazole; L-AMB: amphotericin B liposome; MIC: rice Carfungin; RZF: Rezafungin
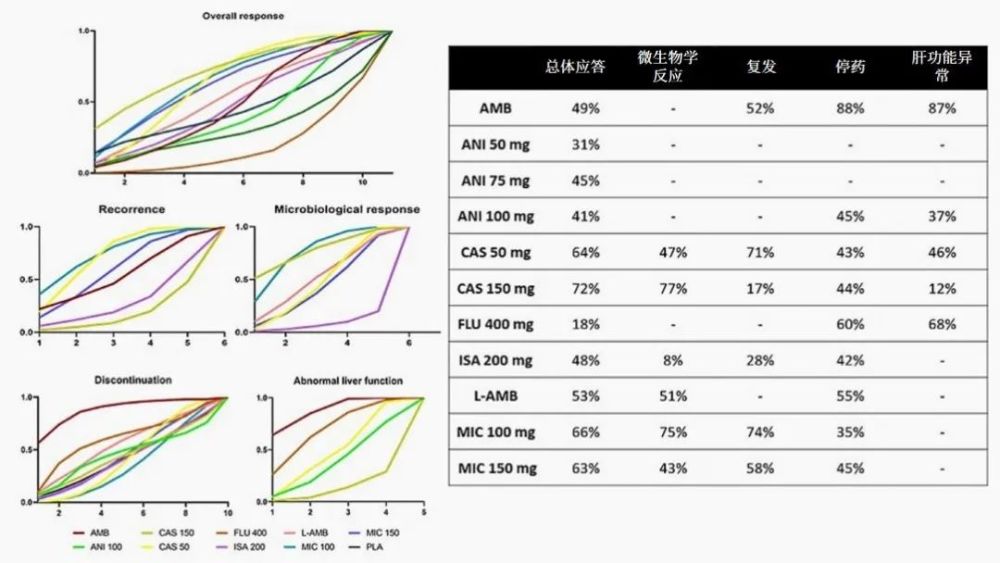
Figure 2 Cumulative Ranking Curve Analysis (SUCRA) Surface Report
Note: Values range from 0% (ie, treatment is less related to outcome) to 100% (ie, treatment is more related to outcome).
Conclusion
The results of this study show that echinocandins are more recommended as first-line treatment for invasive candidiasis, with caspofungin and micafungin in the order of priority. Rezafungin, a new echinocandin in development, is a potential treatment option and should be further investigated in clinical trials. The evidence that azoles and amphotericin B liposomes can be used as second-line therapy in the event of resistance or hypersensitivity reactions requires further study.
References:
Domingos EL, Vilhena RO, Santos JMMF, et al. Comparative efficacy and safety of systemic antifungal agents for candidemia: a systematic review with network meta-analysis and multicriteria acceptability analyses. Int J Antimicrob Agents . 2022 Aug;60(2):106614.