Does your baby have these problems?
Always prefer head tilted to one side;
I like to let you hold breastfeeding on the left side, but I don’t want to let you hold the breastfeeding on the right side;
Lagging behind in gross motor development.
If your baby has the above problems, you may need to consider the problem of torticollis in your child. We will talk about this problem today.
What is torticollis?
torticollis is a symptom, not a diagnosis, clinically characterized by a neck problem that causes the head to tilt to the affected side and the face (chin) to turn to the healthy side side, as shown below.

Image source: Author provided
It should be noted in the definition that which side the head is inclined to is the side of the torticollis. Also note here that the head is tilted and the face (chin) is turned.
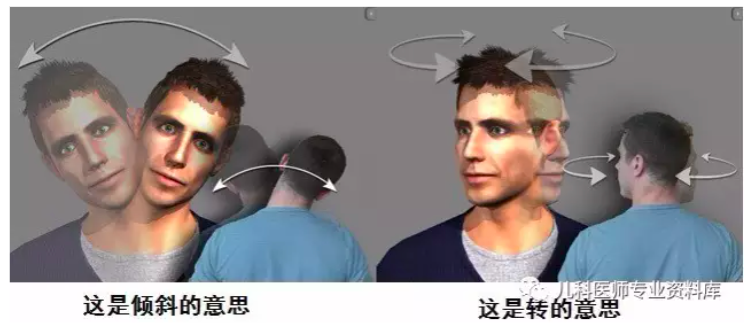
Image source: Author provided
The normal tilt range is that the ears can touch the shoulders, and the normal rotation can reach 90 to 120 degrees in infants, as shown below:
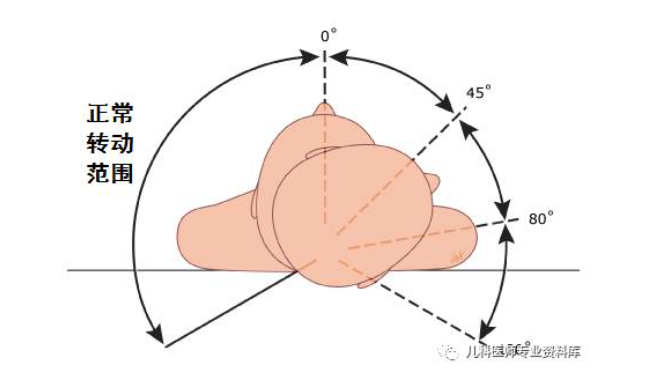
Image source: Author provided
What are the causes of torticollis?
To know why there is a torticollis, you must first know how the neck is not inclined, that is, why the neck is vertical. The neck can stand up, to satisfy:
First of all, the cervical vertebrae are normal, one side cannot be high and the other side is low, and the neck must be upright;
Secondly, the sternocleidomastoid muscle (the main function) and the scalene muscle are symmetrical, and the strength on both sides of the neck is the same, so as to maintain the neutral position of the neck.

Image source: Author provided
The above picture shows the sternocleidomastoid and scalene muscles (3) on the right side of the neck. If they are normal, the muscles are left and right symmetrical to ensure that the neck is upright.
Third, the tissue structure around the neck is normal, and there is no long tumor compressing the muscle or inflammation, which causes one side muscle contracture or pain, causing the neck to lean to one side.
So, if there is a problem with any of the above three points, there will be torticollis:
● Congenital (injury that occurs before birth or perinatal, but may not be discovered until after birth): Congenital problems with the cervical spine, such as The fusion of unilateral atlas leads to a high side and a low side; congenital absence of sternocleidomastoid muscle on one side, spasm of sternocleidomastoid muscle on one side, and cervical web on one side, etc., will all lead to torticollis. The most common congenital cause is spasm of the sternocleidomastoid muscle. This spasm can occur in utero, or it can be damaged during birth.

Image source: Author provided
● Acquired (torticollis that appears gradually after birth, mostly after 6 months of birth): All acquired factors cause the above skeletal and muscle abnormalities, All are acquired, such as neck fractures, osteomyelitis, neck inflammation leading to muscle contractures, abnormal muscle tension, soft tissue tumors, etc. The most common of the acquired are sternocleidomastoid and obliqueInflammation of the quadratus muscle (the outer layer of the back of the neck, prone to injury, inflammation).
The common causes of torticollis are congenital, and acquired are rare.
Because congenital muscular torticollis is the most common, today we will focus on:
Types of congenital muscular torticollis
Congenital muscular torticollis is divided into three types, from mild to severe:
●Posture (light): Only changes in posture (head to one side, chin to the other side), no sternocleidomastoid tension or Mass, no movement restriction. That is to say, the child only likes to tilt his head to one side, but the child tilts his head to the other side, and there is no problem in turning his head.
●Muscular (moderate): The sternocleidomastoid muscle is tight, but the mass is not palpable; neck movement is limited. The child’s sternocleidomastoid muscle is tight to the touch. When the child tilts his head to the healthy side, it will hurt and cry.
● Sternocleidomastoid mass (heaviest): A palpable mass on the sternocleidomastoid muscle restricts neck movement. There is a mass on the sternocleidomastoid muscle. The mass is hard and well-defined. Most of the mass is located in the middle and lower 1/3 of the muscle, and a small part is a hard mass in the upper part or all the muscles. The mass is obvious at 1 to 8 weeks (within 2 months) after birth, and usually resolves automatically by 2 to 6 months of age, but muscle tension and other factors continue to exist.
Manifestations of congenital muscular torticollis
● Mostly manifested in 2 to 4 weeks after birth. Children tend to turn their head to the affected side and their chin to the unaffected side.

Image source: Author provided
● There is no conclusion about whether torticollis is more on the left or on the right. An article in Hong Kong suggests that there are more torticollis on the left (a total of 1086 children were examined), while in Taiwan One article hints that there are more right sides (a total of 197 children were examined), but the ratios are all around 50:40, and there is not much difference. The picture below shows right torticollis, which means the head is turned to the right side of the child and the chin is turned to the left side of the child.

Image source: Author provided
● Severe, prolonged torticollis may lead to plagiocephaly and facial asymmetry, as described below.
● Some children with congenital muscular torticollis have deformities such as developmental hip dysplasia and varus feet. For information on hip dysplasia, you can refer to the article: Is the baby walking normally? Walking posture in developmental dysplasia of the hip.
Congenital muscular torticollis
Changes in head and face shape (which side of the face is bigger?)
One side torticollis can lead to contralateral plagiocephaly, the contralateral ear is moved forward, the contralateral orbit becomes larger, and the contralateral side appears larger, resulting in a smaller torticollis lateral eye fissure.
Why does it cause the oblique head on the opposite side? Take the following picture as an example, with torticollis on the right side, when you sleep, you will use the pillow on the left to touch the bed surface. Over time, the forehead on the left will be pushed forward, and the left occiput will be flattened. As a result, the left ear is moved forward, the left eye socket becomes larger, and the left face appears larger.
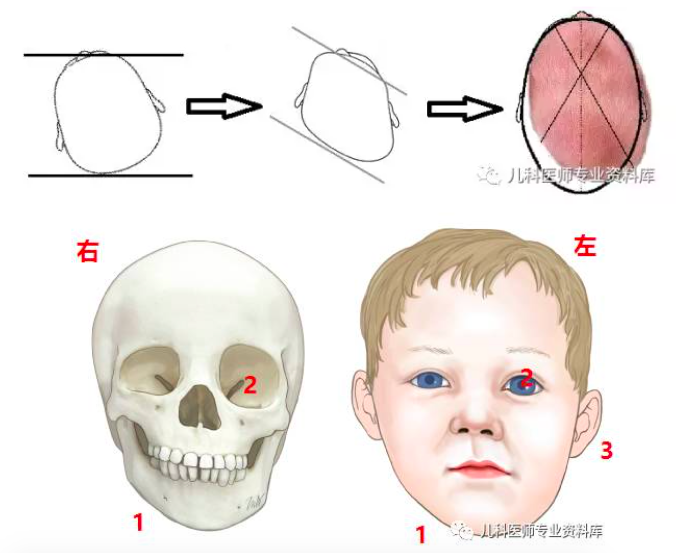
Image source: Author provided
The picture is modified from uptodate, the right side is the torticollis side, which side has the torticollis, which side has the smaller face.
Causes of congenital muscular torticollis
The etiology of congenital muscular torticollis is unknown.
● May be related to abnormal placement of the fetal head in utero (breech-presenting infants have a higher rate of torticollis than top-presenting infants), fibers resulting from damage to the sternocleidomastoid muscle in utero or at birth associated with contractures. Injury to the sternocleidomastoid muscle caused by injury at birth is also congenital.
● Congenital muscular torticollis is genetically linked.
● Always hold the child in one position (for example, always prefer to hold the child on the left side), less prone position when the child is awake, also sleeps in a car seat at home, and always sleeps on one side Aggravated torticollis.
Diagnosis of congenital muscular torticollis
● When the child always likes to turn his head to one side, but is attracted by objects, he can freely turn his head to the other side without squint, craniosynostosis and other problems, can be diagnosed as postural type.
● If the child develops torticollis within 2 to 4 weeks after birth, and can feel a mass on the sternocleidomastoid muscle, or feel particularly tight on one side, prompt Is lumpy or muscular. Ultrasonography can be done if tension, mass, or degree of tension cannot be determined.
● If the child has torticollis and limited activities, but the sternocleidomastoid muscle is not tense and there is no mass, it may not have much to do with the muscle, and the cervical spine needs to be considered The problem needs to be confirmed by X-ray examination.
Progress and prognosis of congenital muscular torticollis
● Congenital muscular torticollis may heal on its own, but it is uncertain how much it will resolve spontaneously. Some severe cases may lead to plagiocephaly and craniofacial asymmetry.
● The earlier the treatment, the better the effect. Studies have shown that if first-line treatment is performed within 1 month after birth, the average treatment can be cured in 1.5 months; treatment after 1 year of age requires an average of It takes about 10 months to be effective. Treatment is better than no treatment. Intervention (passive stretching) performed within 1 year of age, although it takes a long time and the child is uncomfortable, is 90% effective and does not require surgery.
Treatment of congenital muscular torticollis
The purpose is to achieve midline head position, posture and gross motion symmetry, prevent/improve craniofacial asymmetry, and address limitations in neck range of motion.
● After the diagnosis of torticollis, if the baby is older than 6 months, and has persistent neck movement limitation, obvious oblique head and facial asymmetry, it needs to be checked by a surgeon, See if it is necessary to release the sternocleidomastoid muscle to avoid further aggravation of the above abnormalities. And it is recommended to follow up with an ophthalmologist to see if there is any vision problem.
● If the baby does not have the above conditions, the congenital muscular torticollis can be relieved first through posture and physical therapy (stretching).
● Treatment should be carried out under the guidance of a doctor (usually a physiotherapist abroad), the doctor will teach the parents how to treat, and the parents will train the baby at home. If there is no effect after 4 to 6 weeks, it should be A therapist treats.
● The younger the child (eg, less than 2 months), the softer the neck will be and the less autonomous movement it will have, resulting in a more acceptable treatment, easier treatment, and less time , the better the effect. The average treatment time is 4 to 6 months to achieve the curative effect.
Treatment of congenital muscular torticollis
First-line methods include posture and body position; control of environmental factors; passive neck extension; and promotion of active movement.
Adjuvant therapy includes micro-current therapy, massage, the use of soft neck sleeves, etc., because it has not been proven, this article will not go into details.
If first-line treatment is ineffective and surgery is required, this is a surgical problem and is not covered in this article.
1. Postures and Positions: Including holding the child and lying prone when awake.
How to hold a child: For a child with torticollis on the right side, hold the child with the left hand. As shown in the picture below, when the child wants to tilt his head to the right, your left arm just blocks his head, preventing him from tilting his head to the right and turning his head back. A simple memory is that which side of the child’s torticollis is leaning against you, haha.

Image source: Author provided
Prone position when awake (that is, on the stomach): The prone position under adult supervision is very important for the treatment of torticollis when the child is awake. The head will stand up, which stretches the sternocleidomastoid on the affected side and strengthens the neck muscles. Lying down a lot is good for the children’s big sports in the future.
The method is to spend a total of 1 hour a day in the prone position, or at least 3 times a day, each time as long as the child can tolerate. When the child is on his stomach, in order to increase the time, you need to play with the child in front of the child or on the affected side.
2. Controlling environmental factors: The purpose is to let the child turn his face to the affected side in order to see things, so as to achieve the effect of stretching the shortened sternocleidomastoid muscle on the affected side.
Methods are:
The child is placed in the crib so that the healthy side (that is, the side where the chin is turned) is a white wall. Stretch the shortened sternocleidomastoid muscle on the affected side.
When the baby is lying down, put toys on the affected side of the baby, so that in order to see these things, the child will turn his chin to the affected side to stretch the shortened sternocleidomastoid muscle Effect.
3. Passive neck extension
Passive neck stretch is a stretch in the opposite direction based on the performance of your baby’s torticollis. When torticollis, the head is tilted to the affected side and the chin is turned to the unaffected side. When stretching, turn the head to the unaffected side and the chin to the affected side. This can achieve the effect of stretching the sternocleidomastoid muscle on the affected side.
When doing passive stretches, make sure that your child has no cervical spine problems. If you do passive stretches, you will cause further cervical spine damage! How to be sure? If you can feel the sternocleidomastoid muscle mass and tension in the neck, it is basically a muscle problem. If the sternocleidomastoid muscle is normal when you feel the sternocleidomastoid muscle, the child has limited neck movement, and a cervical spine x-ray can be determined.
The earlier you do passive stretching, the easier it is to do, and the better the effect. It is best to do it within 2 months, because the muscles are not tight and easy to stretch. do passive stretchesWhen exercising, the child must not resist. If the child cries and fights you hard, it will damage the neck muscles and be harmful to the child.
In addition, there is no consensus on how to perform passive stretching. Different studies recommend different intensities and frequencies. The following content is based on uptodate treatment of torticollis.
Tilt the head to the unaffected side: Put your baby in a supine or sitting position with one hand immobilizing the baby’s body while the other hand tilts the baby’s head toward the unaffected side so that the ears touch To the shoulder, hold for 10 seconds to 2 minutes (if the child does not make trouble, try to hold on for as long as possible). During this period, in order to keep the baby from crying, talk to the baby and let others tease the child.

Turning the chin to the affected side: Put your baby in a supine or sitting position with one hand immobilizing the baby’s body and the other hand turning the baby’s chin to the affected side so that the chin touches the affected side Side shoulders, hold for 10 seconds to 2 minutes (if the child is not making trouble, try to hold on for as long as possible), during this period, in order to keep the baby from crying, talk to the baby and let others tease the child.
In the above two pictures, the child has a right torticollis, and the chin is turned to the left. During training, the chin should be turned to the right.
Alternate 3-4 repetitions of the above exercises, each time you change your baby’s diaper. The more you do, the longer you persist, and the faster your child gets better.
4. Promote active movement
For small infants, active neck movement can be facilitated by lying on their stomachs (heading their heads) and controlling environmental factors (turning their heads). For older children, that is, children older than 6 to 8 months, children are unwilling to do passive stretching exercises, and active exercise is more important, mainly through righting training, allowing children to lie on their stomachs, and children sitting and guiding them to turn their heads and other methods to promote initiative. sports.
Rightening training: Hold the child from behind, let the child sit up, and then tilt the child to which side to see which side of the child’s torticollis. At this time, In order to ensure that the head is in the neutral position, the child will actively tilt the head to the unaffected side to achieve the purpose of stretching the sternocleidomastoid muscle on the affected side. Hold for a while, if the child is uncomfortable, let the child return to the neutral position, and then repeat the above actions.
The child sits and guides him to turn his head: This is relatively simple, that is, the child sits up, teases the child on the side of the child’s torticollis, and asks the child to turn the chin toward the affected side , to stretch the sternocleidomastoid muscle on the affected side.
Evaluation of treatment effects
After torticollis treatment, follow-up should be conducted every 2 to 4 weeks, 2 weeks in severe cases, and 4 weeks in general. If the torticollis improves every time you visit, you can continue to treat it at home. If it doesn’t improve, you need professional physical therapist treatment.
Signs of successful treatment: no visible torticollis, normal range of neck rotation, symmetrical voluntary movements, motor delivery and age-matched.
Cooperative expert Kong Lingkai
Attending Pediatrician
Master of Pediatrics, Second Military Medical University
Basic Life Support (BLS) Certified Instructor
Review Expert Ma Xuemei
Deputy Chief Physician of PLA Northern Theater General Hospital
This article was first published on the public account “Pediatrician Kong Lingkai” and may not be reproduced without authorization.
Typography: Beautiful
Producer: Astro
The source of the title map: Zhanku Hailuo