Pregnancy and childbirth have changed the mother’s body a lot. What repair efforts have you made after childbirth?
Let’s listen to the mother of Lilac Mother Planet@It’s reassuring*^O^* the story of it.
Foreword Summary
Tell me about my situation first. I had a caesarean section because of a suspected macrosomia + dangling abdomen. I gave birth to 3.95kg, but the estimated weight of the fetus before birth has exceeded 4kg; and I myself, although very fortunate, did not have morning sickness during the whole pregnancy, and I only gained 13kg in a state of good appetite, but the abdominal wall was slack. Prenatal palace height 38cm, abdominal circumference 102cm.

The third trimester had to use a tummy tuck to maintain pelvic stability
How big is your belly? Since the 6th month of pregnancy, it has been that every street and alley, everyone’s mouth, the first sentence they meet is “twins?”, even the doctor in the B ultrasound room will ask this when I enter the door I. I have explained to you countless times that it is not twins, not even the anterior wall, and the amniotic fluid is within the normal range.
Dangling belly also caused a classic misunderstanding, almost everyone who met me during pregnancy believed that I was carrying a son. Because the dangling belly cannot be seen from the back waist, only the belly is very large, and the belly has a “pointy” shape, which is in line with the so-called “male fetus portrait”, um, it really has no scientific basis.
I was about to pack up and go home after my 42-day postpartum check-up. The doctor asked me if I wanted to check the pelvic floor muscles. Although I didn’t have symptoms such as urine leakage, I still adhered to the principle of checking it was not harmful. If it didn’t work, I should repair it as soon as possible. The doctor ordered a pelvic floor muscle function evaluation.
Pelvic floor muscle testing begins
Pelvic floor muscle testing requires emptying the bladder. Lie flat, take off one trouser leg, put your feet on the bed, and bend your legs. Afterwards, similar to a vaginal ultrasound, a soft probe will be inserted. If there is a little discomfort during insertion, the nurse will prompt you to relax. Once inserted, there will be no discomfort. Straighten your legs and bring your knees together to ensure that the probe does not fall off.
I did two assessments, the Supine Muscle Fiber Comprehensive Assessment and the Supine Sexual Function Assessment.
Actually, the process is similar, first contract the muscles as much as possible, and then relax as much as possible to obtain dynamic pressure and static pressure values. Next, you will see a grid with a “channel” on the screen. A bird flew across the screen with a line, and the machine issued commands such as “tighten,” “keep,” and “relax.” All I need to do is to tighten, hold, or relax the pelvic floor muscles according to the instructions, so that the bird on the screen can fly high, maintain a high altitude, or descend, and keep the flight trajectory within the “channel” as much as possible. The value of this “channel” will be between the dynamic pressure and static pressure values obtained before, which is the pressure value that I am guaranteed to reach. The difference between the different assessments is only in the different “channel” graphs.

Graphs on the screen just like the report
(It was a mess the first time)
To be honest, I was pretty confident. Because I have been practicing yoga during pregnancy, I have not done less exercises on the pelvic floor muscles. Where the pelvic floor muscles are and how to exert force, I think I am more familiar than others. Unexpectedly, when I came up, my dynamic pressure was only 40+cmH2O, and 80 reached the passing level. After two sets of evaluations, the problem of muscle explosiveness is not big, that is, it can quickly contract and relax, but it cannot be maintained. The result is that the muscle strength of class I muscle fibers is 0, the damage is more serious, the vitality value is also insufficient, and the synergistic function is slightly damaged. It is recommended to perform pelvic floor muscle function training.
Pelvic floor muscle rehabilitation is here
After seeing the evaluation report, the doctor recommended that I do a 10-course rehabilitation treatment.
Later, I learned that the initial evaluation and the first course of rehabilitation are covered by medical insurance; after the first course of If more courses are needed, re-evaluation and more courses are self-funded items.
Before the treatment, the nurse collected some information, such as age, pregnancy status, whether there were symptoms such as leakage of urine, uterine bulge, etc. Before each treatment, the nurse will also confirm that the bladder has been emptied; after the treatment, the nurse will instruct him to perform Kegel exercises with abdominal breathing after returning home. Before rehabilitation, try not to sit on a low bench or squat, and also avoid movements that increase abdominal pressure, such as squatting, when exercising.
In the process of rehabilitation treatment, I consulted with nurses, and usually with my own practice, one course of treatment can reach the standard of rehabilitation. If it doesn’t work after two courses of treatment, then it may need to be treated by other methods (I don’t know the specifics), and the most patients she knows have only done it 25 times. After recovery, if it is not for high-intensity physical labor, there is generally no problem.
Rehabilitation consists of two parts, one is functional training and the other is electrical stimulation. The former is very similar to the evaluation process, except thatThe shapes passing through the “passage” are different and more diverse, including hillsides with different slopes, stairs and other shapes; the latter is next to the vulva, with electrodes attached to the left and right sides, and electrical stimulation is used. Helps muscles activate and relax. For the first four times, I did functional training first, followed by electrical stimulation. The electrical stimulation was to the degree of pain; the last six times, I did electrical stimulation first, followed by functional training. The intensity of electrical stimulation was just enough to not reach pain. should.
I thought that there would not be too many people who did not pass the pelvic floor muscle assessment, but when I started to do rehabilitation treatment, I found that there were 40+ people in this small second-class hospital during the same period. Pelvic floor muscle therapy, so much so that I only lined up my first treatment two weeks after my evaluation. These 40+ people have just finished giving birth like me, and also have old aunts who look quite young. It seems that the problem of pelvic floor muscles has been taken seriously by many people.
After a month and a half of treatment, my dynamic pressure can fluctuate around 60 and the highest is over 70+. After the re-evaluation, my muscle fiber strength of class I and class II both reached level 5. Although the dynamic pressure is still not qualified, and there is a certain degree of fatigue, after the hand consultation of the chief doctor of pelvic floor muscle disease (that is, the finger is inserted into the pelvis to touch the pelvis). Bottom muscle), after comprehensive evaluation, it is no longer recommended to continue treatment. However, the nurse still told me to continue abdominal breathing + Kegel exercises when I got home.
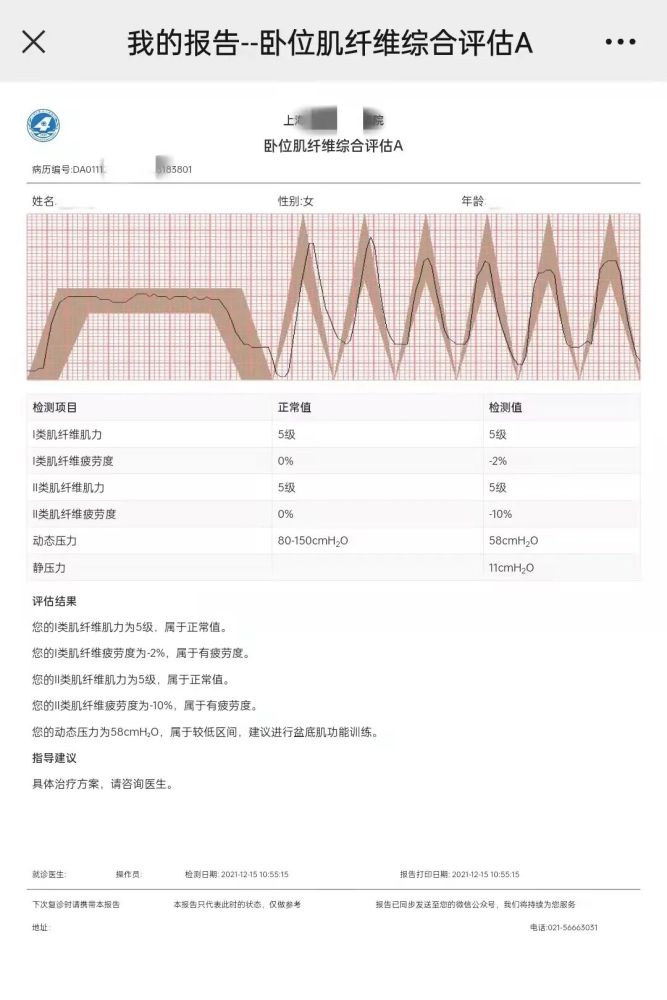
Image source: @ is reassuring*^O^*
Finally, let’s talk about the necessity and suggestions for pelvic floor muscle rehabilitation in the hospital.
As mentioned earlier, I have exercised through yoga during pregnancy and postpartum, and I also have pelvic floor muscle exercises, so what is the difference between the two? Can yoga practice replace therapy? From my personal experience, in fact, the functional training part of rehabilitation therapy is very similar to yoga practice, but it is more specific through the probe and the graphics and values on the screen.
For example, the muscles of the hand are the muscles we use most often. We have a very clear perception of the strength of the grip, but we may still not know how much the grip strength is. number. When you have already grasped tightly, and let you maintain the strength or even tighter, we try to do it, but it may be uncertain whether we have done it, let alone the weaker pelvic floor muscles we perceive. .
Therefore, if it is evaluated by a doctor and recommends pelvic floor muscle rehabilitation, it is best to follow the doctor’s advice, and the degree of damage is relatively minor. It is recommended that you practice daily by yourself. Gel exercises or practice under the guidance of a yoga teacher.
The sooner the pelvic floor repair can begin, the better, which means the busiest time in the postpartum period. If pelvic floor muscle rehabilitation is performed, it is recommended to choose a hospital close to home, which is easier to adhere to. After feeding, go out, each treatment for 40 to 50 minutes, and return home to feed, there is no delay in things, and there is no need to worry about the baby while treating, or suffer from the discomfort of breastfeeding.
Muta

Review Specialist
Zhuozheng Medical Obstetrics and Gynecology Doctor / Former Senior Attending Doctor of Obstetrics and Gynecology Department of Peking University People’s Hospital / High Risk Obstetrics Department