*For medical professionals only
Don’t ignore any details of the patient’s illness~
Foreword Summary
A 31-year-old female patient[1], who was initially admitted to the emergency room with pneumonia, was found to have high blood pressure with new-onset cardiac enlargement. The doctor immediately completed the admission examination, trying to find out the cause of high blood pressure and heart disease.
However, during this period, the patient developed acute kidney injury (AKI) with acute and chronic occlusion of the abdominal aorta. With such a complex and dangerous disease, can you guess what it is?
Case profile
Patient presented to an Australian hospital with respiratory symptoms for 6 weeks. He is generally healthy, with a history of medical abortion and two pregnancies in the past.
Physical examination on admission: Blood pressure 198/120mmHg, heart rate 100 beats/min. There were bronchial breath sounds on the right side of lung auscultation, and the rest of the physical examination showed no abnormality. A chest X-ray on admission showed new-onset cardiomegaly, diffuse bilateral mid-inferior lesions with multiple lateral interstitial lines and pulmonary venous congestion (Figure 1). Chest CT showed ground-glass opacities with mediastinal lymphadenopathy.
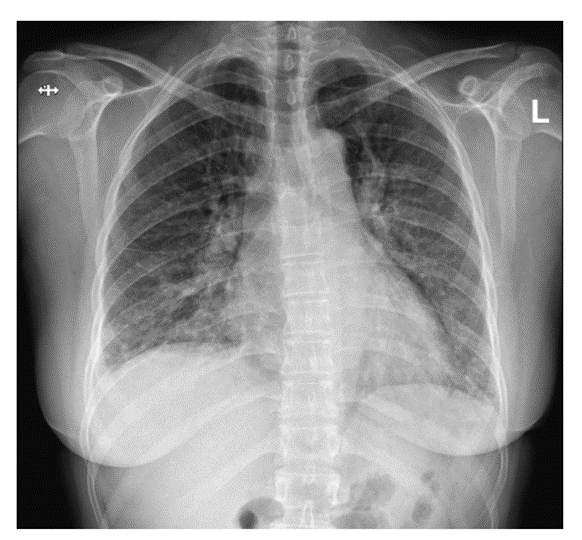
Figure 1 Chest X-ray on admission
Laboratory Testing:
White blood cell count (WBC) 21.3×109/L, C-reactive protein (CRP) 212mg/L and N-terminal precursor b-type natriuretic peptide (NT-proBNP) 16788ng/L high, with a creatinine of 72 mol/L.
Looking deeper, what is the spike indicator?
Seeing this, do you still think that this is a common pneumonia patient, and the patient has indeed started taking azithromycin and ceftriaxone to treat pneumonia. But what is confusing is, what is the relationship between this soaring blood pressure and NT-proBNP value?
The patient then completed echocardiography (TTE) and renal vascular ultrasonography, which showed mild mitral regurgitation and severe systolic dysfunction, with an ejection fraction of 32%. Doctors prescribe diuretics such as ramipril, spironolactone, and bisoprolol.
However, there are a few more tests that get the attention of doctors! The initial renal vascular ultrasound did not reveal any renal artery stenosis. However, aortic occlusion was found incidentally below the superior mesenteric artery.
A CT scan of the abdomen on day 4 of admission confirmed a 7-cm filling defect in the abdominal aorta below the left renal artery and a marked occlusion of the right renal artery. The distal abdominal aorta, thoracic, pelvic, and femoral vessels had extensive collateral formation (Figure 2), suggesting chronic disease. And the patient had previous symptoms of lower extremity lameness.
In addition, the patient’s renin level was elevated to 116 mU/L, consistent with renovascular hypertension.
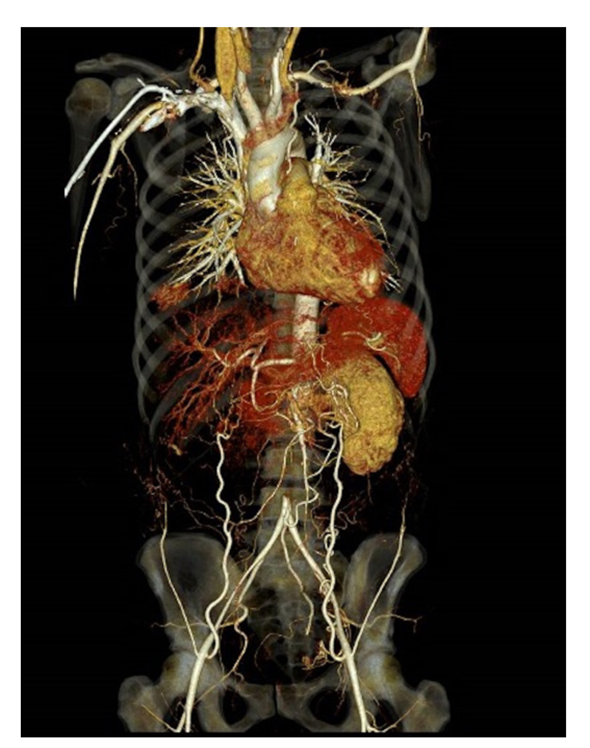
Figure 2 Abdominal CT angiography
Meanwhile, the patient presented with bilateral ear pain associated with discoloration of the pinna (Figure 3), which she had also experienced before.

Figure 3 Relapsing polychondritis
At this point, the initial doubts have not been resolved, and new symptoms have appeared one after another. But in fact, it also provides more basis for doctors to diagnose diseases.
The doctor initially diagnosed large vessel vasculitis and relapsing polychondritis, and the patient was started on pulses of azathioprine and methylprednisolone, which effectively improved the patient’s ear Inflammation. Therapeutic anticoagulation with low molecular weight heparin and screening for causes of vasculitis and thrombosis.
The improvement of the patient’s ear symptoms seems to mean that the disease has begun to develop for the better. Unexpectedly, the patient’s kidneys began to fail before he could feel the joy of seeing the first effect.
It’s complicated and confusing, and it’s a disease that changes when it changes
On day 5 of admission, the patient developed AKI, and her creatinine increased from 72 mol/L on admission to 124 mol/L. And there was no intention to stop, and renal function continued to deteriorate, creatinine increased to 328 mol/L, and progressed to anuria and urinary retention on day 10. Repeat renal vascular ultrasound showed possible aortic occlusionExtending to the peritoneal axis, there is no blood flow in the renal vessels, leading to deterioration of renal function.
What is the situation with this sudden AKI? Everyone was stunned. Has previously diagnosed vasculitis caused AKI? After all, this is the only diagnosis that can be made so far. Could drugs also be the cause of AKI? Of course, there is another object of suspicion: contrast agents.
Exclude only one by one. After doctors stopped nephrotoxic drugs such as diuretics and angiotensin-converting enzyme (ACE) inhibitors, the patient’s kidney function still showed no signs of recovery, and the “suspect” of the drugs was ruled out.
Also, although the use of contrast media may exacerbate kidney damage, especially in the setting of reduced renal perfusion and the use of nephrotoxic drugs. But AKI occurs within 24 hours of contrast, so it is unlikely that contrast was the primary cause of the initial decline in renal function.
That leaves only the “big suspect” vasculitis.
Pull through the clouds and the real culprit behind the scenes is TA
The patient’s anticoagulation therapy was changed to heparin infusion, and he was urgently transferred to a tertiary hospital for re-examination in the departments of interventional radiology, vascular surgery, nephrology, cardiology, and rheumatology. No intervention, such as stenting, thrombolysis, or surgery, was performed for the thrombotic situation due to the high risk. While in the tertiary hospital, the patient underwent a fluorodeoxyglucose (FDG)-positron emission tomography (PET) scan that, to everyone’s shock, showed no evidence of large vessel vasculitis.
What the hell is going on, all the previous evidence points to large vessel vasculitis, but the precise machine has coldly denied this diagnosis. Without a clear diagnosis, it is even more impossible to explain the patient’s AKI, which made everyone gasp. what should we do?
Miscarriage, AKI, soaring blood pressure and NT-proBNP levels… the truth seems to be close at hand.
Shortly after, the patient tested positive for lupus anticoagulant (LA), anticardiolipin antibody (ACA), and anti-beta2 glycoprotein 1 antibody (anti-beta2GP1 antibody). These all point to a disease – catastrophic antiphospholipid syndrome(CAPS).
Disease Knowledge Window
1. What is CAPS?
To understand CAPS, we must first understand what antiphospholipid syndrome (APS) is. APS, also known as Hughes syndrome, is an autoimmune disorder characterized by venous or arterial thrombosis in the presence of positive antiphospholipid antibodies (aPL), or obstetric conditions (eg, miscarriage, fetal death, and preterm birth) .
CAPS is an autoimmune disease characterized by intravascular thrombosis and/or morbid pregnancy and is associated with aPL positivity. It is a specific type of APS characterized by rapidly progressive multi-organ thrombosis and concomitant high titers of aPL, which can lead to disastrous clinical outcomes [3].
Early diagnosis and therapeutic intervention by clinicians are very important to rescue CAPS from multiple organ failure in the short term, and it also suggests the potential value of anti-inflammatory measures such as hormones and immunotherapy.
The clinical manifestations of CAPS vary because they originate from the organ system affected by the thrombus. The kidney is the most commonly affected organ, and the main manifestations are renal insufficiency and proteinuria. Cardiac problems are also common, manifesting as left ventricular insufficiency, valve insufficiency and, less commonly, myocardial infarction.
2. What are the diagnostic points of CAPS?
History of APS or presence of aPL, such as LA, ACA, persistent positive for anti-β2GP1 antibody.
Involvement time of each organ
Histopathological evidence of small thrombosis.
Other manifestations of multiorgan thrombosis and/or microthrombosis.
3. How is CAPS treated?
Triple therapy with anticoagulation, glucocorticoids, intravenous immunoglobulin, and/or plasma exchange is the recommended treatment.
Case Summary
This case is a young healthy woman who was diagnosed with CAPS at her first illness. And about half of APS initially came in the form of CAPS. The patient was screened again for aPL 16 weeks after onset, and the patient’s anti-β2GP1 antibody remained positive. Thus, the previous diagnosis of CAPS was confirmed. The patient subsequently underwent hemodialysis and continued to receive therapeutic anticoagulation and glucocorticoids.
References:
[1]Kwak S, Green M. Rare yet catastrophic presentation of undiagnosed antiphospholipid syndrome[J]. BMJ Case Rep 2022;15
[2]Wang Wenqiang, Li Zhongxin, Kong Xiaolu, et al. Diagnosis and research progress of antiphospholipid syndrome[J]. Massage and Rehabilitation Medicine, 2021, 12(10):3.< /p>
[3] Yang Xin, Li Dengju. Key points and progress of diagnosis and treatment of catastrophic antiphospholipid syndrome [J]. Thrombosis and Hemostasis, 2020, 26(1):4.
Source: Rheumatology and Immunity Channel of the Medical Community
Author: Xianfei
Review: Chen Xinpeng Deputy Chief Physician
Editor in charge: Wang Hang
Proofreading: Zang Hengjia
Plate making: Xue Jiao