It is well known that various chemotherapy drugs have toxic effects on actively growing tissues, and have varying degrees of bone marrow suppression and digestive tract reactions. In order for clinicians to discover and deal with these adverse reactions and side effects in a timely and accurate manner, the author summarizes the side effects and prevention methods that need special attention for your reference.
Myelosuppression
Myelosuppression is the most common hematologic toxicity of chemotherapeutic agents, and the degree and duration of reduction are related to the type of chemotherapeutic agent, dose, combination therapy, and patient-specific factors.
Risk factors for myelosuppression
The occurrence of myelosuppression after chemotherapy is not only related to the chemotherapy regimen, but also to the patient’s own factors, for example: advanced age receiving full-dose chemotherapy, bone marrow invasion, liver and kidney function Abnormalities, immunosuppressive state, recent surgery, previous radiotherapy and chemotherapy, etc., need to be considered comprehensively.
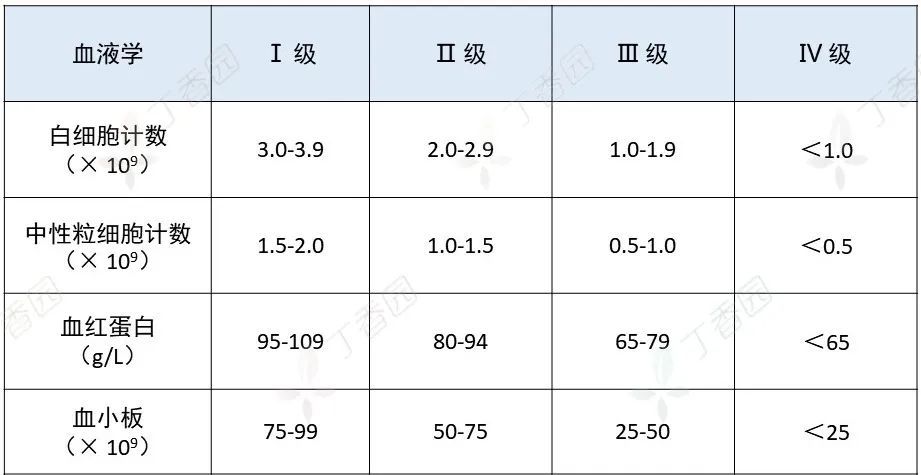
Bone marrow suppressionGrading of suppression
Myelosuppression is classified into 4 grades according to the NCI-CTCAE 5.0 criteria:
MyelosuppressionManagement
For patients at high risk of febrile neutropenia (FN), prophylactic use of G-CSF is recommended; for patients with low to moderate risk, prophylaxis is not recommended and can be G-CSF was administered after neutropenia.
hemoglobin
Treatment of chemotherapy-related thrombocytopenia includes platelet transfusions and administration of platelet-stimulating growth factors. Platelet growth-stimulating factors include recombinant human interleukin 11 (rhIL-11), recombinant human thrombopoietin (rhTPO), the TPO receptor agonists romistatin and eltrombopag.
Currently, only rhIL-11 and rhTPO are approved by the State Food and Drug Administration for the treatment of tumor-related thrombocytopenia in mainland China.
In the event of CIT and bleeding symptoms, platelet transfusions or rhTPO should be given at the same time as platelet transfusions;
In the event of CIT but no bleeding symptoms, platelet count ≤ 10×109/L, prophylactic platelet transfusion or rhTPO should be given at the same time as platelet transfusion;
Platelet transfusion is not recommended when the platelet count is greater than 10×109/L.
Nausea
Chemotherapy Induced Nausea and Vomiting (CINV) is a common, usually predictable and preventable adverse effect of chemotherapy.
For chemotherapy patients, CINV prevention and treatment should be considered in the first cycle. Prevention of CINV during the first chemotherapy cycle reduces the risk of expected CINV in subsequent cycles of chemotherapy.
CINVrisk factors
Patient characteristics: Female, under 50 years old, history of low-dose alcohol intake, history of motion sickness, history of morning sickness during pregnancy, previous history of CINV, anxiety.
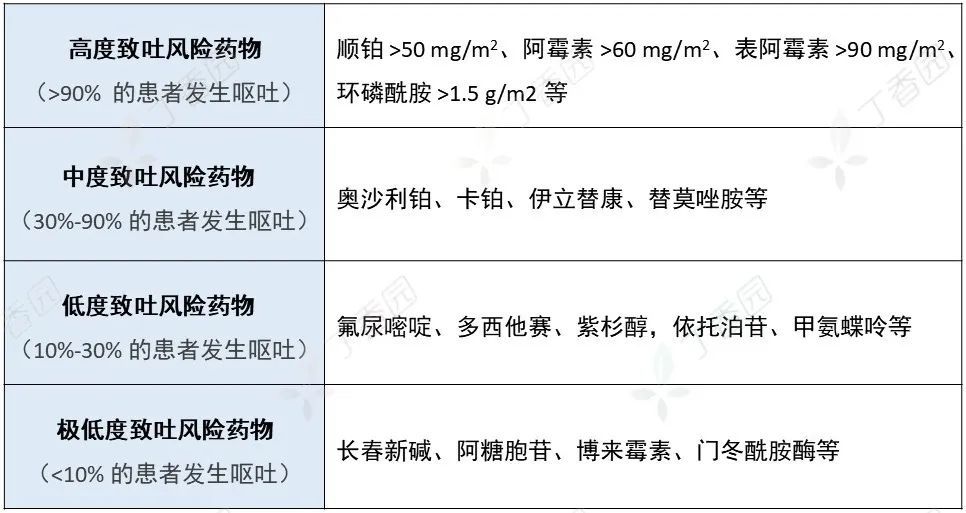
Chemotherapy: use of an emetic regimen (see below for emetic risks), short IV infusions, repeated cycles of chemotherapy, etc.
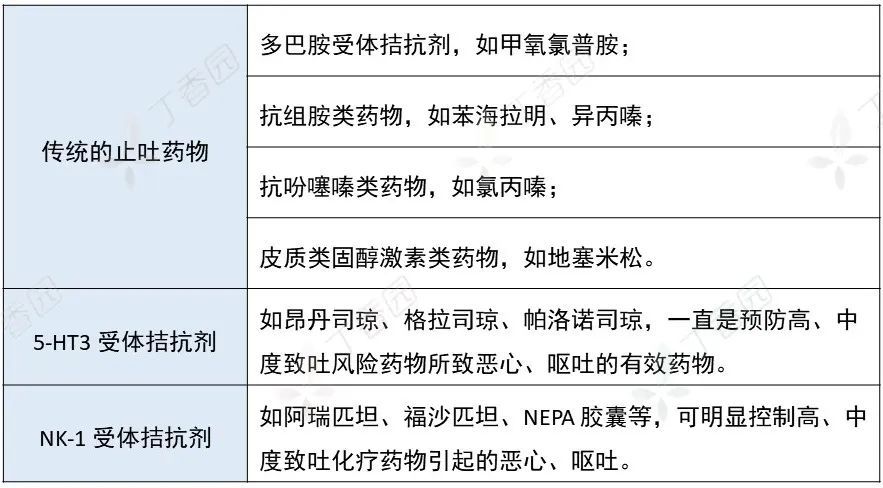
CINVtherapeutic drugs
CINV handling strategies
For patients receiving high emetic risk chemotherapy regimens, 5-HT3 receptor antagonist + NK-1 receptor antagonist + dexamethasone Triple regimen, or quadruple regimen of 5-HT3 receptor antagonist + NK-1 receptor antagonist + dexamethasone + olanzapine.
For patients with moderate emetogenic risk chemotherapy regimens, 5-HT3 receptor antagonists + NK-1 receptor antagonists (including carboplatin) or 5-HT3 receptor antagonists + Dexamethasone (without carboplatin regimen) for antiemetic therapy.
bellydiarrhea
Chemotherapy-induced diarrhea (CID) is a common gastrointestinal side effect caused by chemotherapy in cancer patients. CID will not only reduce the quality of life of patients, but also lead to water and electricity disorders, dehydration, infection, and severe shock and death.
The most common drugs that can cause CID are fluorouracil and irinotecan, as well as hydroxycamptothecin and capecitabine.
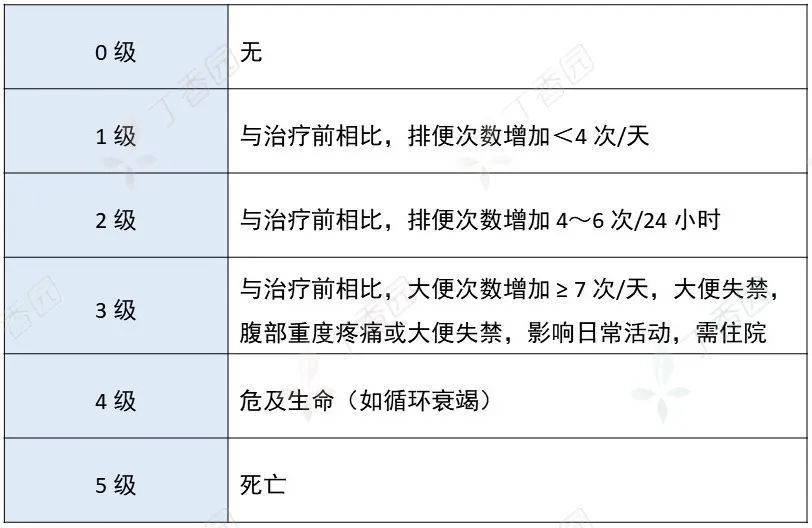
CID Rating
According to the grading scale of the International Cancer Society, CID can be divided into grades 0-5:
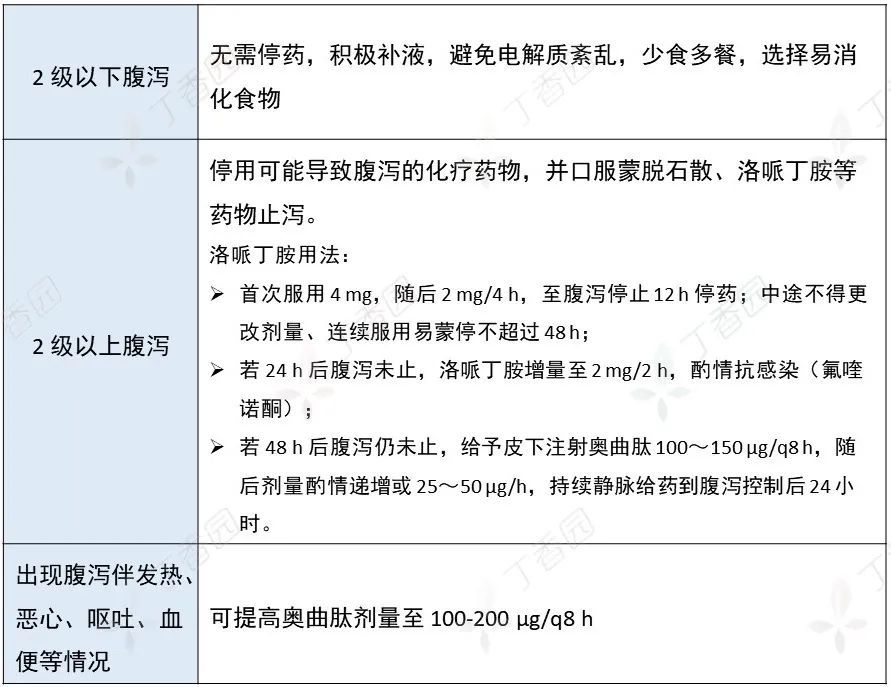
Handling of CIDs
Before the use of irinotecan, the incidence of diarrhea can be roughly predicted by testing the UGT1A1 gene, homozygous mutant UGT1A1 7/7, heterozygous UGT1A1 6/7, wild type UGT1A1 6/ 6. The incidence rates of grades 3-4 delayed diarrhea were 27.6%, 18.5%, and 6.9%, respectively.
There is no need to prevent diarrhea before chemotherapy, just stop laxatives (lactulose, etc.), and give different treatments according to the different grades of diarrhea after chemotherapy:
cardiactoxicity
Different antitumor drugs have different manifestations of cardiotoxicity, which can be divided into:
Cardiac impairment (eg, anthracyclines and trastuzumab)
Vascular impairment (eg, 5-FU and capecitabine)
Injury to cardiac function and blood vessels (eg, bevacizumab and sunitinib)
Chemotherapy can either directly lead to heart disease, or contribute to or be an important risk factor for cardiovascular disease.
Cardiotoxicity
Anthracyclines have a significant dose-response linear relationship on cardiac damage, and their cardiotoxicity is also closely related to the cumulative dose. Different tumor patients have different susceptibility to cardiotoxicity caused by anthracyclines, and some patients can show cardiotoxicity when they are used for the first time, so there is no absolute “safe dose”.
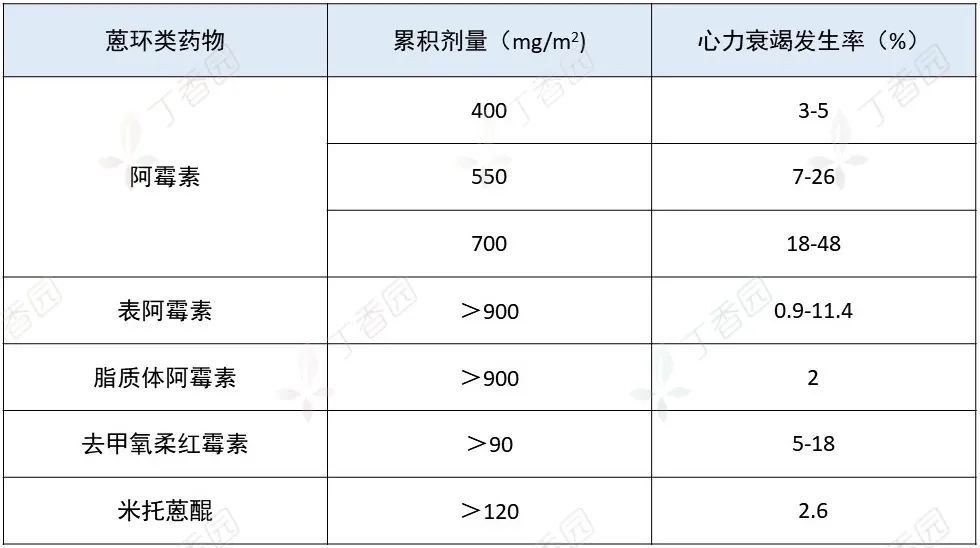
Maximum cumulative dose of anthracycline cardiotoxicity
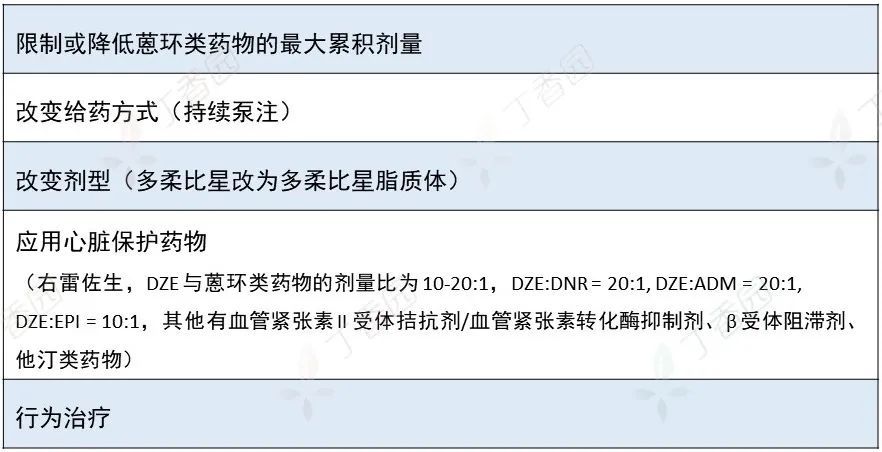
Cardiotoxicity prevention
Drug-inducedLiver injury
Chemotherapeutic drugs and their metabolic excipients may induce abnormal liver function, namely drug-induced liver injury (DILI), also known as drug-induced liver disease.
Chemotherapy drugs that may cause DILI include: cyclophosphamide, cyclosporine, methotrexate, oxaliplatin, etc.
Risk factors for DILI include: advanced age, female sex, pregnancy, alcohol consumption, combined use of drugs, chronic liver disease, AIDS, etc. .
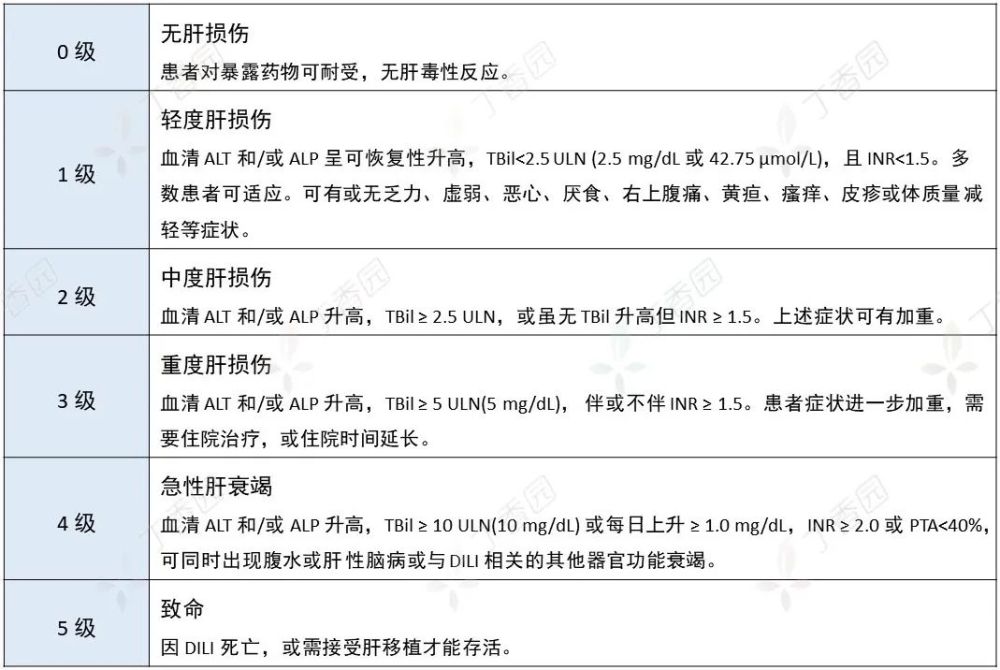
DILI Severity Rating
DILI Handling Principles
The primary treatment for DILI is the prompt discontinuation of the drug suspected of causing liver damage, which may be discontinued or reduced in doses for intrinsic DILI.
In order to avoid the risk of abruptly discontinuing the drug, which may lead to aggravation of the primary disease, the discontinuation criteria in FDA drug clinical trials can be used as a reference (one of the following):
Serum ALT or AST>8 ULN
ALT or AST>5 ULN for 2 weeks
ALT or AST>3ULN and TBil>2ULN or INR>1.5
ALT or AST >3ULN with progressive fatigue and gastrointestinal symptoms, and/or eosinophilia (>5%)
Hepatoprotective drugs (magnesium isoglycyrrhizinate injection, diammonium glycyrrhizinate enteric-coated capsules, etc.) can be given early.
Peripheral neurotoxicitysexual
Clinical commonly used antitumor drugs such as platinum, taxane and vinca alkaloids can induce chemotherapy-induced peripheral neuropathy (CIPN). The incidence of CIPN depends on the type of chemotherapy drug and cumulative dose, and is more common in patients with pre-existing nerve damage (previous history of CIPN or other causes such as diabetes).
Chemotherapeutic agents that may induce CIPN
CIPN Handling Principles
Reduce the dose of chemotherapy drugs. Studies have shown that when peripheral neurotoxicity occurs with taxane drugs, the dose needs to be reduced by 20%; for peripheral neuropathy caused by cisplatin and other drugs, prolong the chemotherapy interval, reduce Chemotherapy dose is a necessary measure;
For CIPN caused by oxaliplatin, patients should pay attention to keeping their hands and feet warm;
Administration of drugs that nourish nerves, such as mecobalamin.
Hair lossHair
Chemotherapy drugs that can cause hair loss
Policy of Handling
Psychological counseling should be actively carried out, and patients are advised to cut their hair short, wear a wig, and inform that the hair can grow back after chemotherapy.
References:
1. Shi Yanxia, Xing PR, et al. Expert consensus on the diagnosis and treatment of neutropenia caused by tumor chemotherapy (2019 edition) [J]. Chinese Journal of Oncology, 2019(17).
2. Shi Yanxia, Xing PR, Zhang Jun, et al. Expert consensus on diagnosis and treatment of chemotherapy-related thrombocytopenia in China (2019 edition) [J]. Chinese Journal of Oncology, 2019(18):923 -929.
3. Jiang Wenqi, Ba Yi, Feng Jifeng, et al. Chinese expert consensus on the prevention and treatment of nausea and vomiting associated with cancer drug therapy (2019 edition) [J]. Chinese Journal of Medical Frontiers (electronic edition) 2019 Volume 11 Issue 11, Pages 16-26, ISTIC, 2019.
CSCO Guidelines for the Prevention and Treatment of Anthracycline Cardiotoxicity, Version 4.2020
5. Yu Lecheng, Mao Yimin, Chen Chengwei. Guidelines for the diagnosis and treatment of drug-induced liver injury [J]. Chinese Journal of Viral Diseases, 2015.
6. Li Junling. Management of chemotherapy-related adverse reactions [J]. Cancer Progress, 2015(6):569-569.
Planning: GoEun, Mei Zhe
The source of the title map: Zhanku Hailuo PLUS
This article was first published on the professional platform of Lilac Garden: Tumor Time