I will talk to you today about “reverse triggering”. It occurs from time to time in clinical practice. How to identify it and its clinical significance during mechanical ventilation?
One, the type of man-machine confrontation
“Man-machine asynchrony” or “patient-ventilator confrontation”, referred to as man-machine confrontation, is mainly a phenomenon in which mechanical ventilation is not synchronized with the patient’s spontaneous breathing. The root cause is various factors Abnormal human-machine relationship that leads to the uncoordinated operation of the ventilator and the patient’s spontaneous breathing.
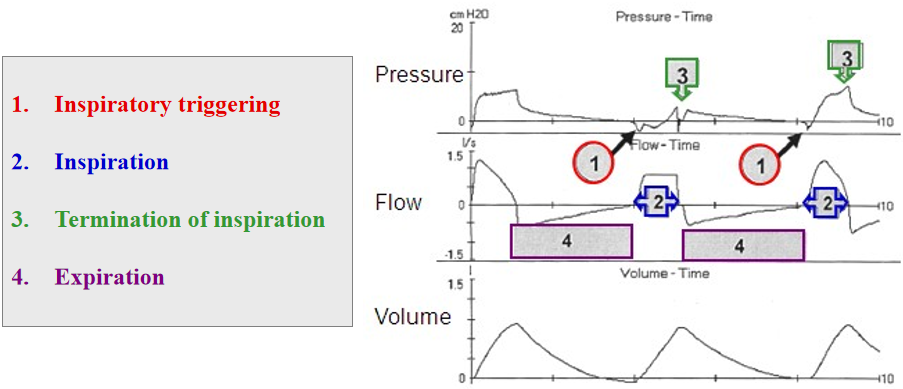
It is not uncommon for human-machine asynchrony to occur. It can occur in the 4 stages of our breathing, such as Inspiratory triggering, Inspiration, Inspiration and exhalation. Termination of inspiration, and Expiration phases.
Second, the mechanism of reverse triggering
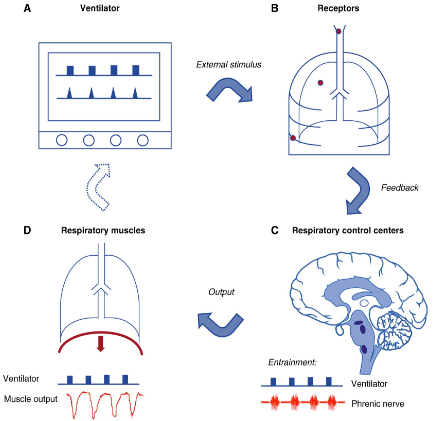
Reverse triggering is actually a manifestation of human-machine asynchrony, which mainly occurs in the inspiratory phase. First of all, let’s look at the “concept” of reverse triggering, which is actually in the controlled ventilation mode , it is the ventilation process of the ventilator that induces the patient’s respiratory center to emit a new breathing rhythm, or a breathing rhythm that is coupled to the mechanical ventilation cycle to a certain extent. This phenomenon is called Respiratory Entrainment, also known as “Respiratory Entrainment” Reverse trigger”.
It is essentially the re-setting of the breathing rhythm by the breathing center of the body under the influence of the periodic ventilation of the ventilator, so as to maintain a stable relationship between the two temporarily. At present, Reverse triggering is still a type of human-machine asynchrony that we are far from fully aware of.
There are several concepts in reverse triggering:
1. Entrainment ratio:
Entrainment ratio is the proportional relationship between the mechanical cycle and the neural breathing cycle. 1:1 means 1 machine-controlled ventilation corresponds to 1 neural breath, and 1:2 means 2 machine-controlled ventilations. Ventilation corresponds to 1 neural breath, and so on. Among them, 1:1 is the most common and most stable, and usually lasts for a long time, while 1:2 is easily interrupted by non-entrainment breathing every 10 to 12 breathing cycles. By changing the breathing rate setting of the ventilator, tow characteristics can be changed (eg from 1:1 to 1:3), or the presence of tow can be eliminated entirely.
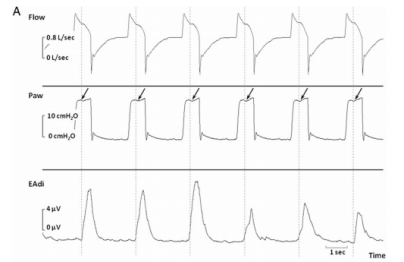
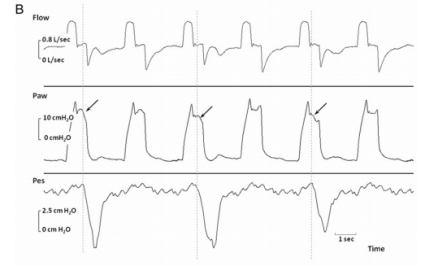
(Picture A tow ratio 1:1, B tow ratio 1:2)
2. Breath stacking:
The patient’s inspiratory effort occurs at the end of the ventilator’s tidal volume output, resulting in a rapid second ventilator delivery. May cause the ventilator to deliver significantly more gas than the set tidal volume. It can be a form of reverse triggering, or it can be “double inhalation”.
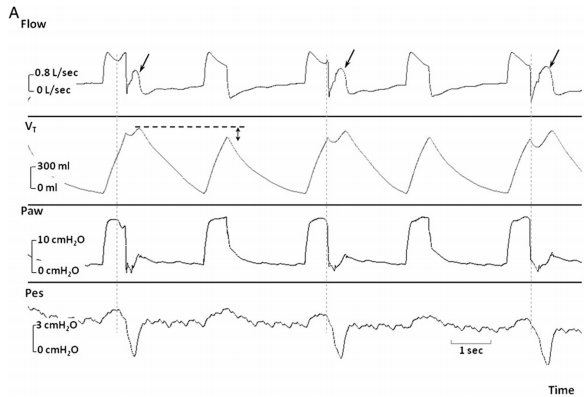
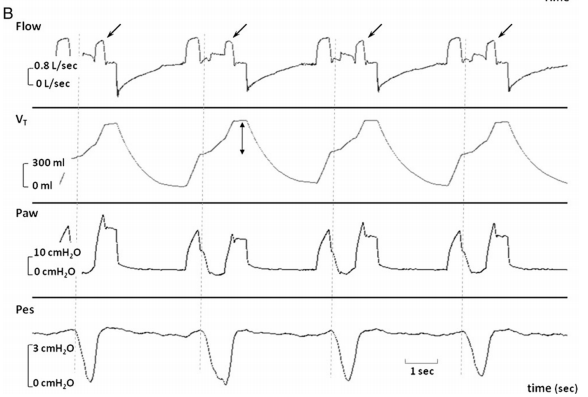
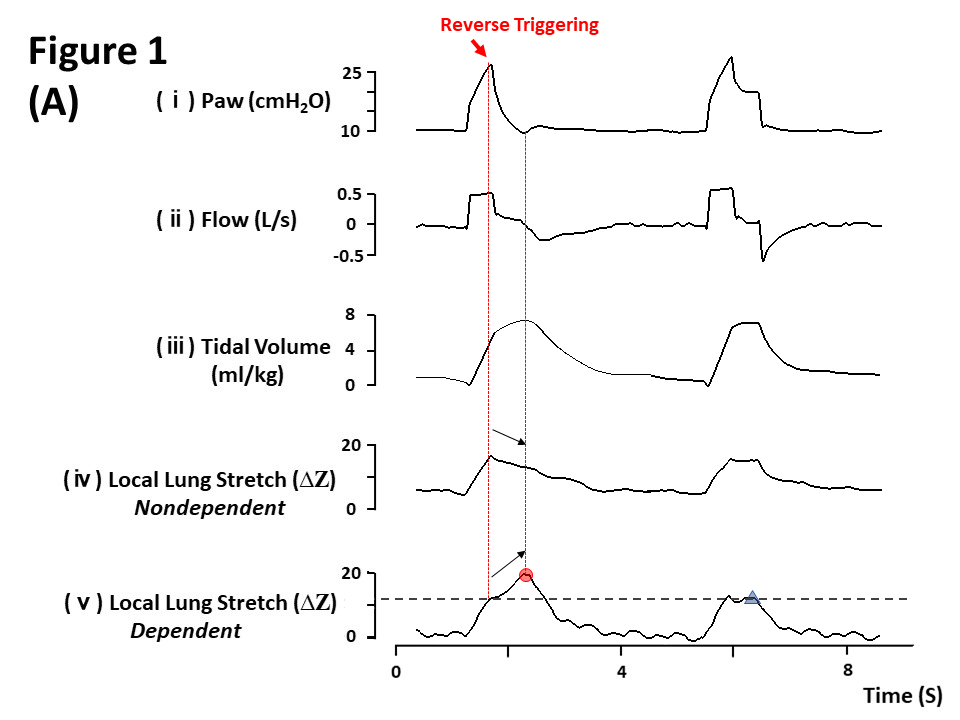
(In Figure A, we can see that reverse triggering causes the tidal volume to increaseplus)
3. Phase difference (dP):
is the time lag between the neuro-respiratory cycle and the start of the mechanical ventilation cycle, in seconds (s). Considering the different lengths of periods, the phase angle (the phase angle, θ), a standardized expression, can more accurately reflect the relationship between the two. The calculation formula of θ is: θ=dP/Ttotmech×360°.
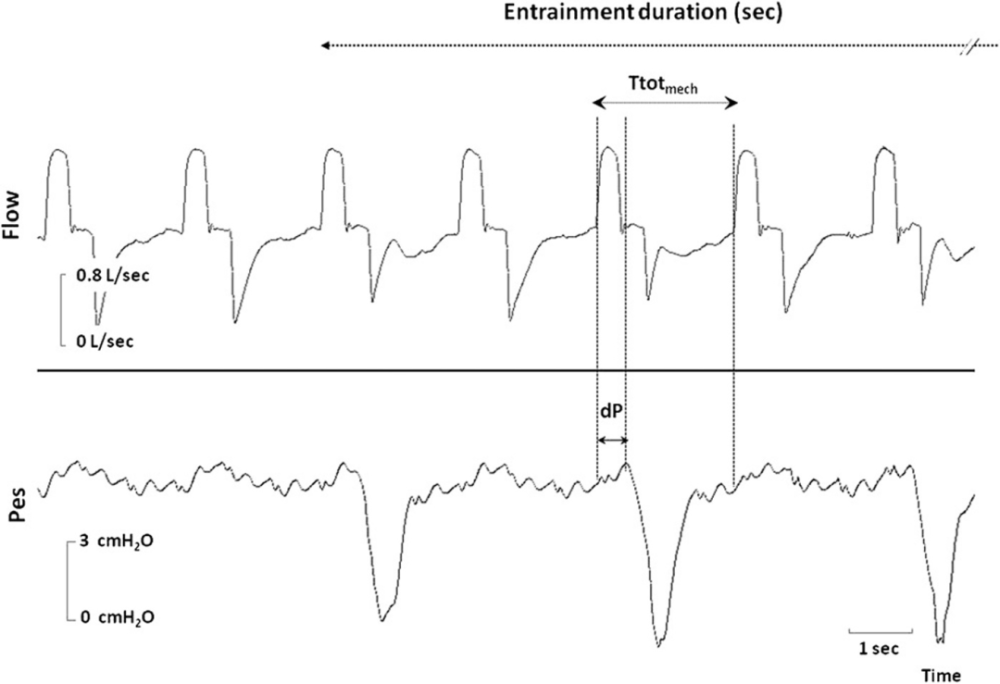
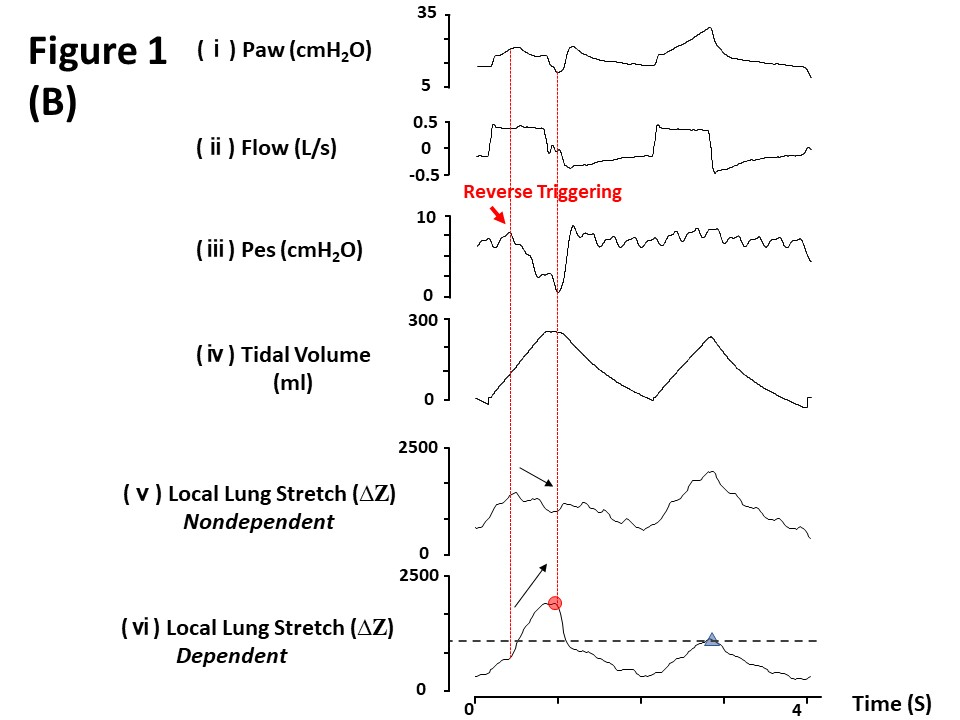
(This picture is a schematic diagram of respiratory drag. Comparing the flow velocity waveform and the monitoring of intraesophageal pressure, it can be determined that the drag ratio is 1:2. In this case, the drag duration is 32.17s, and the phase difference is 0.66s, and the mechanical cycle duration is 2.29s. The calculation of the phase angle is θ=dP/Ttolmech × 360°=104°.)
Third, how to identify reverse trigger?
Reverse triggering is difficult to identify based on waveforms alone, but it is still possible to find clues by carefully observing the various waveforms of the ventilator.
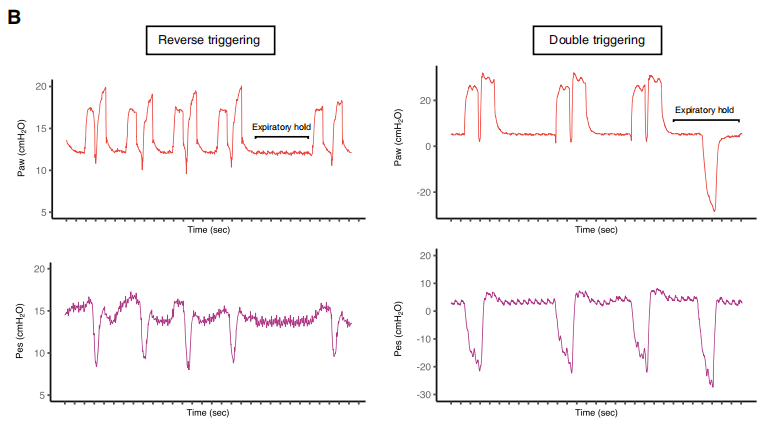
Reverse trigger, or double trigger? The effects of reverse triggering and double triggering are very similar. 1/3 of double triggering is reverse triggering, but the pathophysiology between the two is different, and 5s expiratory block operation can be used to distinguish and identify them. Reverse-triggered breathing occurs in a steady and repetitive manner. Giving a 5s expiratory block maneuver suppresses external stimuli, thereby interrupting respiratory entrainment and preventing reverse triggering. With a 5s expiratory block, the spontaneous effort of the reverse-trigger patient will disappear, while the spontaneous effort of the double-trigger patient will continue and be more intense.
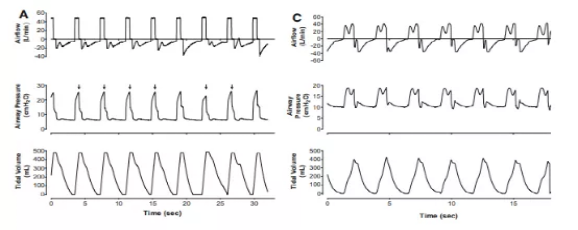
A 2021 article in Chest, a multicenter observational study, incidence of reverse triggers in early ARDS:


(The image above shows an example of a patient respiration waveform with reverse triggering out of sync. Flow, Airway Pressure (Paw), and Esophageal Pressure (Pes) recordings for an ARDS patient. These dots indicate that the script is based on flow and Paw detect the exact time of the reverse trigger. The ratio of ventilator to patient effort is 1:1, and the shallow circles represent the stack of breaths related to the reverse trigger. The inspiratory effort of patients who cannot trigger the rear of the ventilator is represented by the dark circles. )
Study results showed that 50 subjects detected at least one single reverse trigger event during recording, with an asynchrony rate of 4.8 (0.3-14.3) beats/min or accounting for controlled breathing 17.7% of frequency (0.95-49.5). RT without breath stacking and RT with breath stacking were 4 (0 – 12) times/min and 0 (0 – 1.5) times/min, respectively, and RT without breath stacking accounted for 97.3% (80.5-100), the most common The entrainment ratios are 1:2 and 1:1.
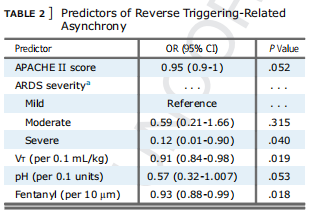
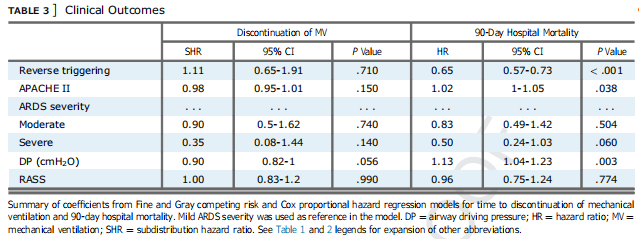
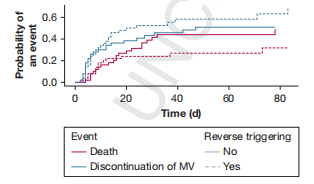
This study also observed that RT was independently associated with lower tidal volume (VT) (P=0.019) and lower fentanyl infusion rate (P=0.018) than Low VT and opioid doses increased the likelihood of developing RT; in addition, greater ARDS severity (p=0.08), higher pH (p=0.053), and lower APACHE II score (p=0.052), The higher the likelihood of RT; also, the presence of early RT was not associated with time to MV discontinuation and, after adjustment for known predictors, may be associated with a reduction in 90-day in-hospital mortality, a presumption that could imply that RT is beneficial to patients An increased chance of spontaneous breathing may be “beneficial”.
This is also a 2021 article, published in Am J Respir Crit Care Med:
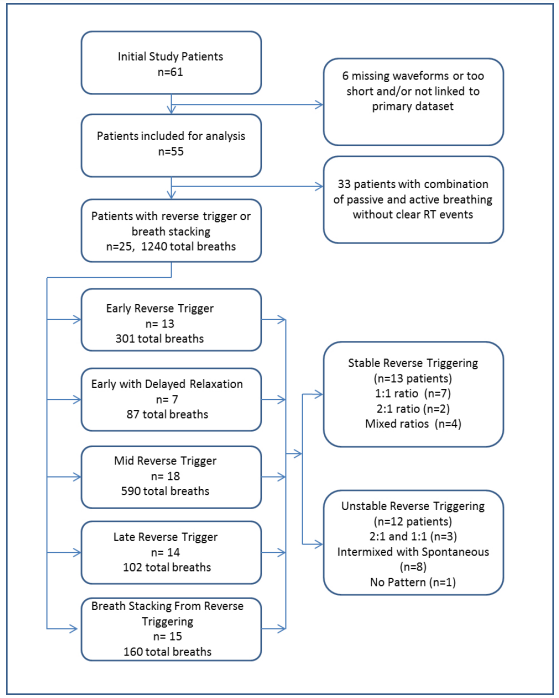
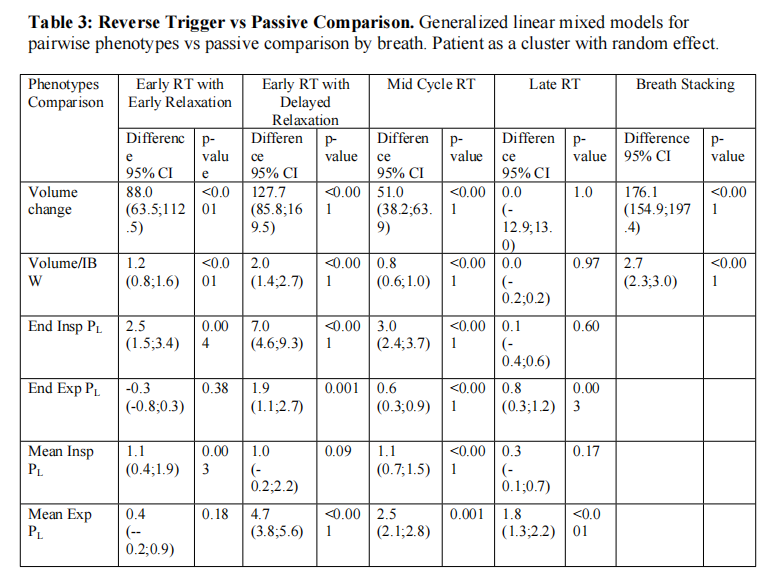
This study collected ventilator waveform data from 55 ARDS patients using pressure-regulated volume-controlled ventilation (PRVC) mode to explore the four RT phenotypes with or without respiratory overlay, and Effects on patient inspiratory and expiratory phases.
Consists of an average of 7.0 (4.5-8.5) minutes per patient for a total of 384.7 minutes and 10266 breaths; of 1240 total breaths (12.1%) in 25 patients (45%) RT and respiratory overlay events were found, with RT with respiratory overlay occurring in 15 patients (27%) of 160 total breaths. Mid-stage RT was the most common phenotype, and RT frequency varied widely. RT occurred with an increase in inspiratory drive (mean 4-10 cmH2O).
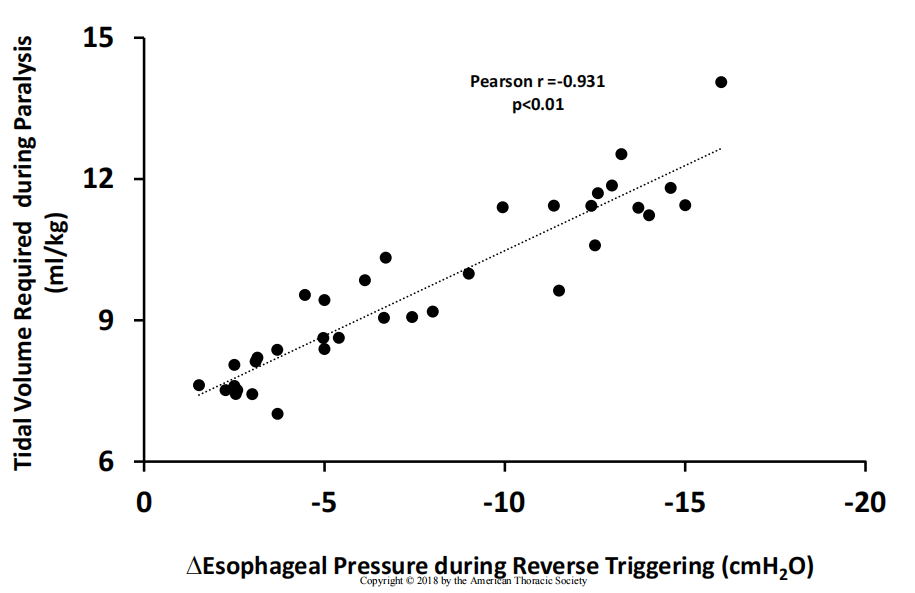
Found that pre-RT increased tidal volume [88 (64-113) ml], inspiratory non-transpulmonary pressure [3 (2-3) cmH2O]; patients with pre-RT with delayed expiration Tidal volume increases [128 (86-170) ml], end-inspiratory and mean end-expiratory transpulmonary pressures [7(5-9) cmH2O, 5 (4-6) cmH2O], respectively; Vapor phase, but maximal inspiratory effort was in the expiratory phase) increased tidal volume [51 (38-64] ml], increased non-inspiratory and mean end-expiratory transpulmonary pressures by 3 (2-4) cmH2O, 3 (2 -3) cmH2O], accompanied by insufficiency; late RT (appearance of expiratory phase) increases the mean expiratory transpulmonary pressure [2(1-2) cmH2O], and leads to insufficiency. Expiratory superposition can lead to tidal volume Add【176(155-197)ml】.
IV. Reverse trigger and lung injury
Reverse triggering may be benign, or even beneficial, to some extent in patients at low risk of lung or diaphragm injury. First, reverse-triggered spontaneous breathing can increase the patient’s muscle activity; second, reverse-triggered active contraction or delayed relaxation during expiration may increase mean expiratory pressure and prevent full expiration, thereby acting as a micro-recruitment mechanism. effect.
However, reverse triggering can also easily lead to lung injury. The main mechanism may be out of synchronization with the superposition of breathing caused by reverse triggering, resulting in excessive tidal volume and excessive transpulmonary pressure. It may also be related to shear stress (pendulum effect) damage caused by the movement of gas across different lung regions when inspiratory effort is too strong.
5. How to deal with reverse trigger?
1. Sedation and analgesia:
Opioids can affect the respiratory center, and the combination of sedatives and opioids can provide comfort, control pain and dyspnea in patients receiving mechanical ventilation, which can help improve patient and Ventilator interaction. Common asynchrony can be treated with sedation and analgesia, but deep sedation is associated with longer duration of mechanical ventilation and ICU stay and is an independent risk of ineffective inspiratory effortfactors, so there are pros and cons.
One study reported a decrease in respiratory stack rate from 41% to 27% when sedation was added in patients with high asynchrony rates, and it was also reported that when sedation was interrupted, the rate of respiratory stack increased .
Reverse triggering can trigger a high airway pressure alarm, usually prompting an increase in clinical sedation, or a ventilator adjustment. In the early stages of ARDS treatment, increased sedation and/or the use of NMBA may be the preferred options.
2. Ventilator settings:
Reverse triggering originates from breath entrainment, so modifying the entrainment mode can limit reverse triggering.
Theoretically, modifying the entrainment frequency can also affect minute ventilation and carbon dioxide levels, which in turn affect respiratory drive. It is speculated that the reverse trigger frequency is also related to the respiratory rate.
Changing the breath rate on the ventilator can alter the entrainment characteristics or eliminate entrainment, so increasing the forced breath rate can eliminate the patient’s neural effort and disrupt the breath drive, and decreasing the forced breath rate may Causing the patient to initiate effort prior to mechanical inflation also effectively eliminates entrainment.
3. Others:
Because of different flow and pressure delivery controls, patients respond differently to the ventilator, and the impact of other ventilator modes including volume control, PRVC, pressure control also requires further study, while the reverse Other factors contributing to triggering need to be further explored. The persistence of the reverse trigger pattern over time and its prevalence across the patient population are also uncertain.
Final summary
Reverse triggering during mechanical ventilation is a human-machine asynchrony that is not fully understood. It can cause secondary triggering, superposition of breaths, resulting in increased tidal volume and transpulmonary pressure. Aggravated ventilator-associated lung injury. But to a certain extent, reverse triggering is also beneficial. Reverse-triggered spontaneous breathing increases the patient’s muscle activity, and secondly, reverse-triggered active contraction or delayed relaxation during expiration may increase mean expiratory pressure and prevent full exhalation, which can act as a micro-recruitment of the lung.
About the reverse trigger, more clinical identification, processing and research are needed, please criticize and correct it.
References (swipe up and down)
[1]Jeremy RB, Atul M, Taylor TB. Ventilator-induced lung injury. Clin Chest Med, 2016, 37(4): 633-646.
[2]Arthur SS, Marco RV. Ventilator-induced lung injury. N Engl J Med, 2013, 369(22): 2126-2136.
[3]Laurence V, Frédéric V, Jean R, et al. Patient-ventilator asynchrony during non-invasive ventilation for acute respiratory failure: a multicenter study. Intensive Care Med, 2009, 35 (5): 840-846.
[4]Evangelia A, Aissam L, Nathalie R, et al. Mechanical ventilation-induced reverse-triggered breaths: a frequently unrecognized form of neuromechanical coupling. Chest, 2013, 143(4) : 927-938.
[5]Pablo OR, Norberto T, Sebastián F, et al. Prevalence of reverse triggering in early ARDS: results from a multicenter observational study. Chest, 2021, 159(1): 186 -195.
[6]Jose D, Michele B, Ewan CG. Monitoring patient-ventilator interaction by an end-expiratory occlusion maneuver. Intensive Care Med, 2020, 46(12): 2338-2341.
Professional Profile

Luo Hong
Professor, Chief Physician, Doctoral Supervisor, Director of the Department of Respiratory and Critical Care Medicine and Director of the Subspecialty of Respiratory Critical Care, Second Xiangya Hospital of Central South University. Member of the Respiratory Critical Care Group of the Respiratory Medicine Branch of the Chinese Medical Association, member of the Respiratory Physician Branch of the Chinese Medical Doctor Association, Deputy Director of the Critical Care Medicine Working Committee of the Respiratory Physician Branch of the Chinese Medical Doctor Association, and member of the Standing Committee of the Pulmonary Rehabilitation Committee of the Chinese Disabled Persons Rehabilitation Association and ICU Deputy head of the Pulmonary Rehabilitation Group, President of the Respiratory Physician Branch of the Hunan Medical Association, and Deputy Director of the Respiratory Rehabilitation Committee of the Hunan Medical Association.
This article was organized and typeset by Jerry, Editor of Breathing World
End of this article
Please do not reprint without permission
Follow us