*For medical professionals only
What’s wrong with the ECG?
Message from the Director

Hello, everyone! I am Li Xuebin, Director of the Cardiac Electrophysiology Department of the Heart Center of Peking University People’s Hospital. ECG is an important auxiliary examination, it must be combined with clinical and disease, in order to play the greatest role and bear the most beautiful fruit. Without the clinical foundation, the ECG is like a flower without soil and rhizomes. No matter how beautiful it looks, it will not last long.
In recent years, intracardiac electrophysiology technology has developed vigorously, which has brought great progress in the diagnosis and treatment of arrhythmia.Intracardiac electrophysiology is like the “pathological result” of ECG Likewise, the ability to dissect the ECG provides the final definitive diagnosis for complex ECGs. “ECG Anatomy Room” aims to connect ECG with disease, diagnosis and treatment, and tell you the story behind ECG.
The challenge is waiting for you!
Case Challenge
Everyone is familiar with pacemakers. Generally speaking, pacemakers are an important device for the treatment of bradyarrhythmias (excluding special pacemakers such as ICD and CRT) ). Bradyarrhythmia patients can quickly correct their bradycardia after implanting a pacemaker, and they can return to work and life normally without long-term medication. Therefore, pacemaker implantation has become an indication. important treatment for patients with bradyarrhythmias.
So, do all patients with symptomatic bradycardia require a pacemaker?
If you need to list extreme cases here, I think everyone can find counter-examples soon: for example, the patient/family disagrees; the patient is in the terminal state of the disease and has a life expectancy of less than 1 year. But what about a patient without the above? Let’s take a look at the case below.
A 50-year-old middle-aged male was admitted to the hospital due to fatigue for more than 1 year. The patient’s fatigue lasted for more than 1 year, especially during activities. The patient had no chest tightness, chest pain, dizziness, and black eyes. Symptoms, occasional arrhythmia, repeated ECG examinations showed bradycardia, echocardiography showed no obvious abnormality. After admission, an electrocardiogram (Figure 1) showed bradycardia, blood pressure 90/50 mmHg, heart rate 37 beats/min, negative cardiopulmonary and abdominal examination, and no edema in both lower extremities.
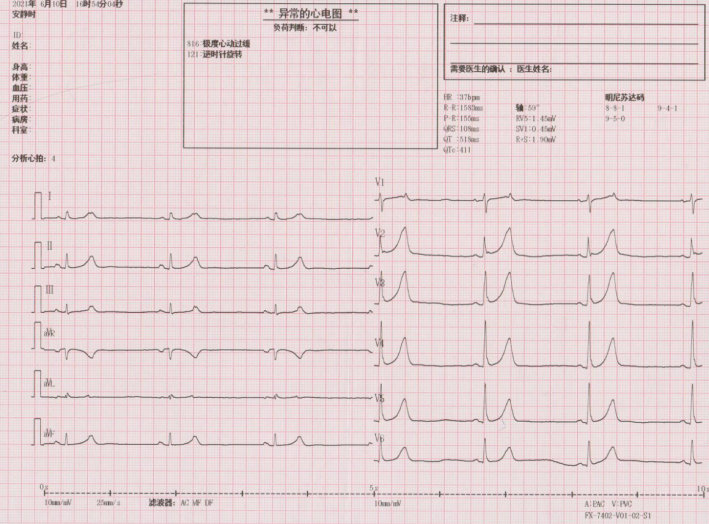
Figure 1: Patient presents with fatigue and ECG shows extreme bradycardia.
What should we do next for such a patient?
Question 1:What is the patient’s basal heart rhythm?
Question two:Is this a slow or fast arrhythmia?
Question 3: Is there an indication for pacemaker implantation?
Question 4: Possible problems after pacemaker implantation?
Question 5: How to further treatment?
You can stop here to think about it, and then continue to read our analysis below~
Case Analysis
Our question may seem a bit extreme, but in fact, this is not an uncommon problem clinically, and we hope to give you a comprehensive understanding of the problem, rather than raising the bar.
Returning to the patient in this case, a 50-year-old middle-aged male, the main complaint is fatigue, which is obvious after activity, and the heart rate is significantly slowed down, and the slow heart rate is significantly related to the patient’s symptoms of fatigue. Therefore, the main clinical problem of the patient can be summarized as symptomatic bradycardia. From this perspective, there is no doubt that the patient should have a pacemaker implanted to increase the heart rate. In this way, a series of symptoms caused by slow heart rate, especially fatigue after activity, can be relieved.
If it was such a straightforward one-way thinking, it would not be a case for us to discuss together. I personally think that we have so many bright minds that it is worth discussing more esoteric clinical issues. Before we officially get back to the question above, let’s go around in circles and ask ourselves, what exactly is the reason for this patient’s slow heart rate?
Looking at Figure 1, someone must have simply pointed out that this is simply sinus bradycardia? Severe sinus bradycardia just explains the patient’s fatigue, especially the symptoms of fatigue after exercise. Severe sinus bradycardia is also one of the manifestations of sick sinus syndrome. Into a pacemaker, from symptoms to ECG and treatment…perfect.
Wait! If we distract our attention a little at this time, noticing the sharp waveform on the T wave in lead V1 (blue arrow in Figure 2), will immediately react that this sharp waveform is not a QRS The wave is not a T wave, nor a U wave, nor interference, so it can only be a P wave, and this P wave is different from the P wavelength of sinus rhythm, then it is arrhythmia, and there is no QRS wave behind the arrhythmia. , indicating that Fang Zao arrived very early, encountered the refractory period of the atrioventricular node, and was not transmitted. The current heart rhythm is called sinus rhythm atrial premature doublet, but Fang Zao has not been transmitted. Although ambulatory early is not passed down, it has a compensatory interval. The appearance of this compensatory interval causes the heart rate to slow down and also causes the patient’s symptoms.
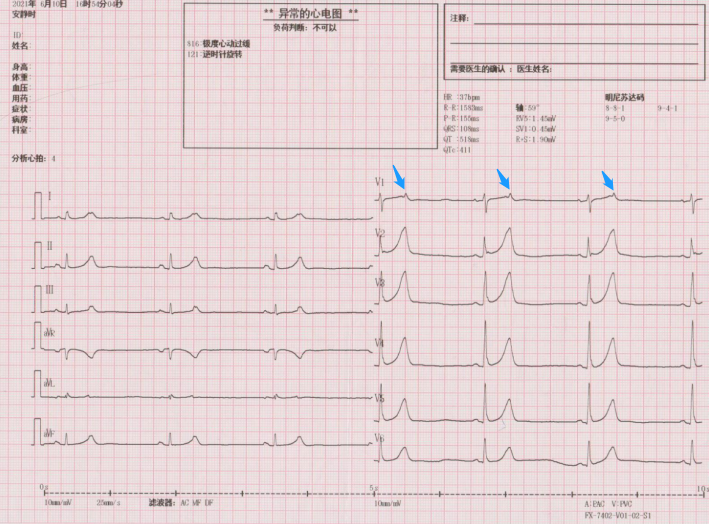
Figure 2: Patient presents with fatigue and ECG shows extreme bradycardia.
So for this arrhythmia, if it is a slow arrhythmia from the perspective of QRS wave or mechanical contraction of the heart; but if from the perspective of P wave, frequent atrial arrhythmias Early, this should be a rapid arrhythmia. If we analyze from the perspective of causality, the slowed QRS wave is the result, and the frequent occurrence of early morning sickness is the cause. In order to solve the problem, we can start from the downstream effect, but we should grasp the upstream cause. Therefore, compared with implanting a cardiac pacemaker and eliminating atrial arrhythmia, eliminating atrial arrhythmia is more thorough and clever.
Assuming that a pacemaker is implanted, the patient is in sinus rhythm and should be implanted with a dual-chamber pacemaker. After the dual-chamber pacemaker can be implanted, its working mode is atrioventricular Versatile pacing (DDD), which senses the electrical activity of the atrium and triggers the electrical activity of the ventricle. The atrial pacing will be converted into ventricular pacing before it is transmitted. The patient is likely to be due to the rapid and frequent heart rate ventricular pacemaker and feel ill.
The P wave above the patient’s lead V1 is upright, suggesting that it originated from the left atrium. After puncturing the atrial septum, using a multipolar mapping catheter, we pinpointed the origin of the atrial anomaly at The anterior edge of the mitral valve (Fig. 3), after ablation at the mapped origin, the atrial prematureness disappeared, the compensatory interval after the atrial prematureness also disappeared, and the patient’s heart rate also increased (Figure 4), and the symptoms of fatigue no longer appear.
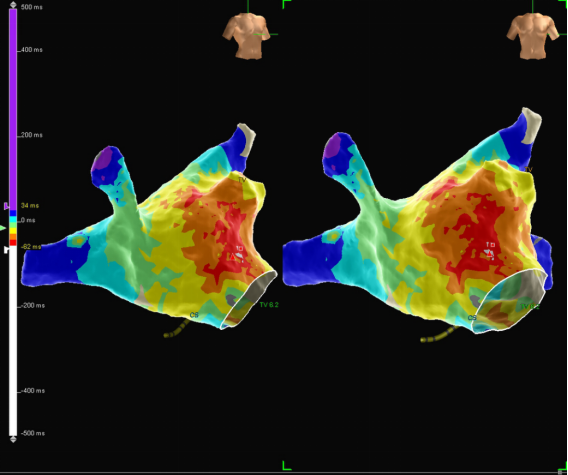
Figure 3: The electrophysiological multipolar mapping catheter was used to map the origin of the atrial arrhythmia from the anterior edge of the mitral valve. The white dots in the figure represent the origin of the atrial arrhythmia.
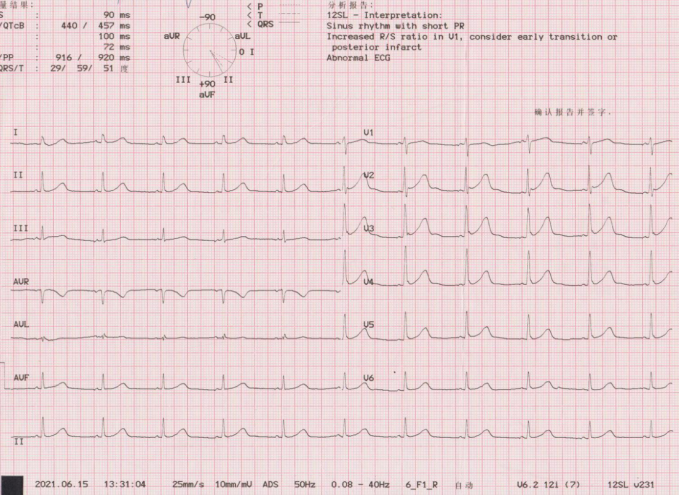
Figure 4: After the disappearance of atrial arrhythmia, the patient’s heart rhythm returned to normal, the heart rate increased, and the strange sharp wave no longer appeared on the T wave in lead V1.
Look, the heart rate is slow, isn’t it necessary to implant a pacemaker? To solve problems, starting from the source is often the most effective!
Professional Profile

Professor Li Xuebin
Li Xuebin, Chief Physician, Doctor of Medicine, Doctoral Supervisor. He is currently the director of the Cardiac Electrophysiology Department of the Heart Center of Peking University People’s Hospital. He has been engaged in the diagnosis and treatment of arrhythmia for a long time, and has completed more than 10,000 cases of catheter radiofrequency ablation and cardiac pacemaker operations. The minimum age is 10 months and the maximum age is 100 years old. He has guided hundreds of domestic hospitals to carry out cardiac interventional operations, covering all parts of the country except Tibet, and has been invited to North Korea for many times to perform operations and guidance. He was the first in China to conduct research on automatic threshold capture pacemaker, three-chamber pacemaker, and right ventricular dual-site cardiac pacing. National CRT Technology Promotion and Popularization Award. In view of his achievements in the field of atrial fibrillation catheter ablation, he was awarded the Outstanding Contribution Award by the Chinese Society of Cardiac Electrophysiology and Pacing. Editor-in-chief and translation of many academic monographs, published hundreds of papers, including more than 10 SCI papers, as the main person in charge, completed more than 20 lectures of the advanced seminar on cardiac electrophysiology and pacing of the national continuing education project, “New Concept Electrocardiography” “More than 20 phases have trained a large number of professionals in cardiac electrophysiology and pacing for our country.

Dr. Ho Jinshan
He Jinshan, an eight-year doctoral student at Peking University School of Medicine, is under the tutelage of famous electrophysiological experts Professor Guo Jihong and Professor Li Xuebin. In addition to mastering the diagnosis and treatment of common diseases in cardiology, under the guidance of Professor Guo and Professor Li Conduct in-depth research on arrhythmia, electrocardiogram and intracardiac electrophysiology, and like to express complex and boring knowledge in a simple and humorous form. He has been a columnist in the “Medical Cardiovascular Channel” for more than 1 year, and has published in domestic and foreign journals such as “Circulation”, “Chinese Journal of Cardiovascular Diseases”, “Chinese Journal of Cardiac Pacing and Electrophysiology” and “Chinese Journal of Cardiovascular Diseases”. Published multiple articles.
References:
[1]The only EKG book you’ll ever need(sixth edition), Malcolm S. Thaler.
[2] Clinical Electrocardiography 5th Edition, Huang Wan.
[3] Zhou’s Electrocardiography 6th Edition, translated by Guo Jihong.
[4] Electrocardiography, edited by Guo Jihong.
This article was first published: Cardiovascular Channel of the Medical Community
This article was written by He Jinshan
Review expert: Prof. Li Xuebin
Editor in charge: Yuan Xueqing, Zhang Li
Copyright Notice