Because of the good density contrast of the lung, it is one of the most suitable examination sites for X-ray. The air content of the lungs and the intrapulmonary pressure are also different due to the breathing movement, so the images of the inspiratory phase and the expiratory phase will be different, and the HRCT of the lungs will show more obvious. It is necessary to pay attention to the breath phase when reading the film. Unless a specific disease is identified, we generally ask for an inspiratory image of the patient.
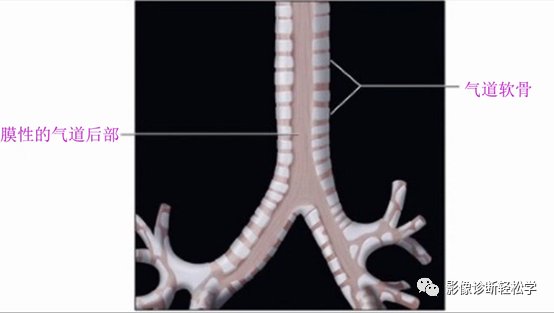
Figure 1 Large airway structure
The effect of breathing on the density of large airways and lungs
The posterior part of the large airway is a membranous part without cartilage support and is easily affected by airway pressure. In normal people, the posterior wall of the airway becomes flat during exhalation. (Fig. 2a) In patients with tracheomalacia, airway narrowing was most prominent in the anteroposterior diameter of the trachea and increased transverse tracheal diameter, features that were more pronounced during expiration. (Fig. 2b) Lung density increases during expiration due to the reduction of air in the lungs. (Figure 2b)
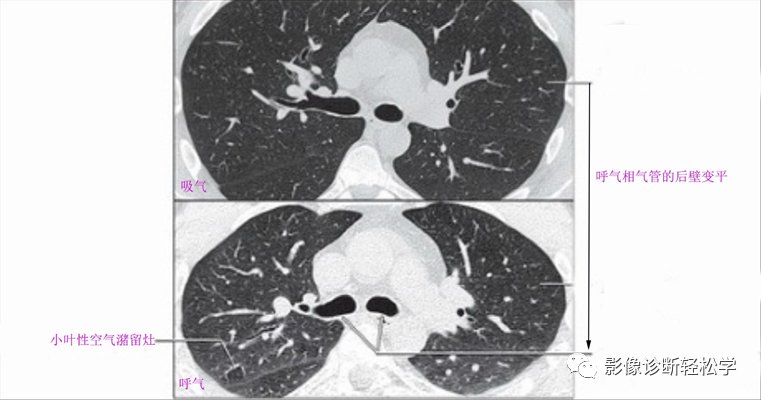
Figure 2 a
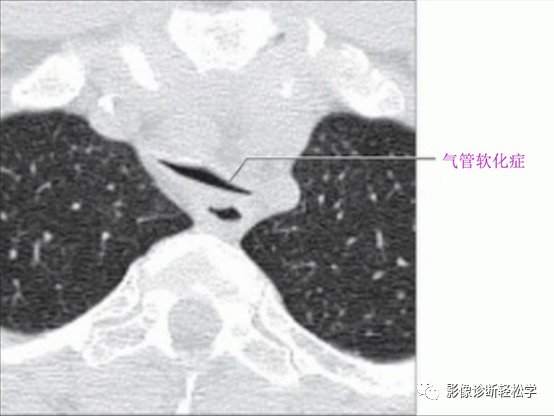
Figure 2b
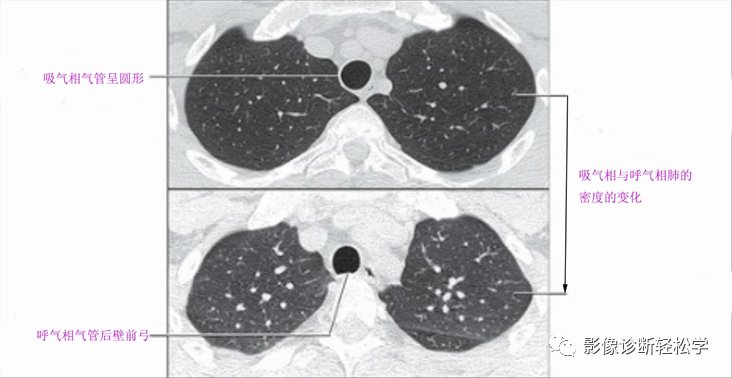
Figure 2c The increased density of the lung can be seen in the expiratory phase
Most of the time, the quality of the image is compromised when the patient is not breathing well. affect the diagnosis of lung disease. Especially for GGO nodules in the lungs, the images of the inspiratory and expiratory phases have a significant impact on the judgment of the size and density of the nodules. Expiratory imaging is sometimes required: for example in diffuse and focal airway obstruction and small airway disease, expiratory phase is better. (Expiratory phase is collected during pause after full exhalation)
Example: Coronal expiratory HRCT in patients with restrictive bronchiolitis shows air trapping, mosaic density and mosaic perfusion. Note that the diameter of the pulmonary vessels is larger in the hyperdense regions than in the hyperlucent lung parenchyma. Expiratory HRCT in patients with a near-normal inspiratory phase shows obstructive changes. (Picture 4)
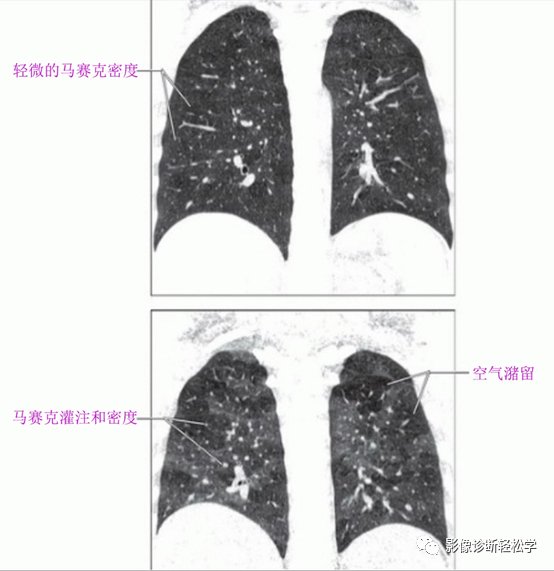
Figure 4 (Note: Only a slight mosaic density can be seen in the inspiratory phase in the upper image. The lower image Lesion is more obvious in expiratory phase)
Abnormal expiratory image: mosaic perfusion (Fig. 4)
1 Inhomogeneous lung density
2 Air Decreased perfusion in the retention area
3 The blood vessels are smaller in the (abnormal) hypodense lung area compared to the (normal) hyperdense lung area.
Identification:
Mosaic density (Fig. 4)
Lung density was uneven, and there was no sensory difference in pulmonary vessel diameter.
Air trapping on expiratory imaging (Fig. 4)
Increased lung density with scattered abnormal hypodense foci during normal exhalation.
References:
“HRCT of the Lung”