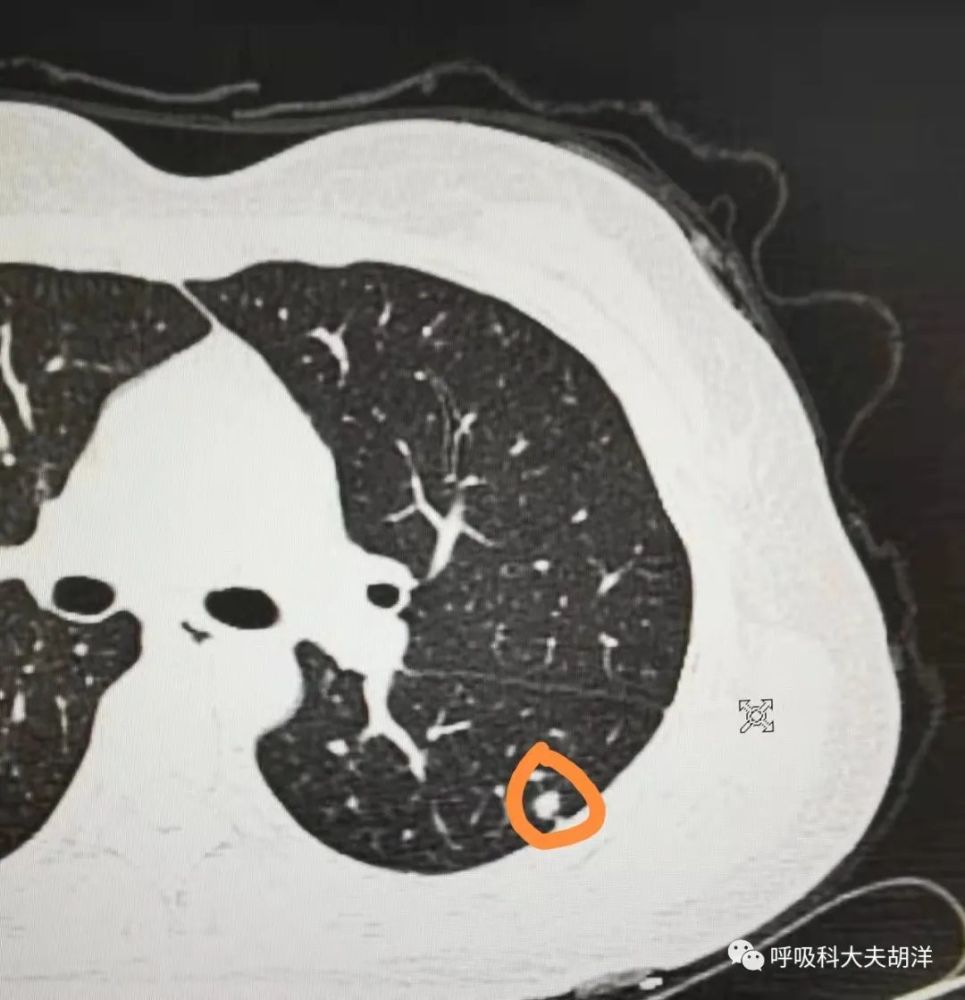
A 41-year-old female presented an 8mm nodule on chest CT during a routine physical examination at the unit. From the image, this nodule has burrs, lobulations, and has pleural traction. Since it is a solid nodule and is close to the pleura, it may develop more rapidly if it is malignant. However, the nodule was too small to be punctured, so doctors in the local hospital suggested direct surgical excision. However, when the pathological results came out, the patients were both happy and worried. The happy thing was that the pathology was inflammatory pseudotumor, not lung cancer. The worry is that removing part of the lung because of a benign nodule seems to be a bit of a loss.
Inflammatory pseudotumor disease has been discussed many times before. As the name suggests, it is a tumor-shaped nodule or mass formed by inflammation, not a real tumor. It can only be regarded as a benign disease, a chronic, non-specific, proliferative inflammation, so it is not even a benign tumor. When there is inflammation and infection in the lungs, some can be completely absorbed, and some can not be absorbed and form scar tissue, which is manifested as fibrous shadows and calcifications. Some chronic inflammation gradually produces granulomas and chronic proliferation, forming a nodule or mass shape in the lungs, which is inflammatory pseudotumor.
Inflammatory pseudotumor can occur in both men and women. It is more common in people over the age of 40, usually in the right lung. Most inflammatory pseudotumors are asymptomatic. A small number of patients with large inflammatory pseudotumor and poor location close to the hilum of the lung may have symptoms similar to lung cancer, such as low-grade fever, chest pain, cough, expectoration, and blood in the sputum.
Why are inflammatory pseudotumors mistaken for lung cancer and undergo surgery?
The main reason is that inflammatory pseudotumors on imaging are very similar to lung cancer. On CT, inflammatory pseudotumor can also appear as soft tissue density shadow, and there are also malignant signs such as lobulation, burr, vascular connection, cavitation, etc., and even enhanced scan will show enhancement. Some inflammatory pseudotumor lesions are located around the hilum, similar to central lung cancer, so it is sometimes difficult to distinguish and identify them by CT alone.
Theoretically, for lesions highly suspected of malignancy, routine lung puncture or bronchoscopy is recommended to clarify the pathology. However, some lesions are too small to be punctured, and some patients are so anxious that they request surgery as soon as possible but suffer from heart disease. For various reasons, every year, a very small number of patients are suspected of being malignant but the surgical pathology is a benign disease.
Inflammatory pseudotumor is a proliferative foci formed by chronic inflammation. Generally speaking, once a pseudotumor is formed, it is extremely unlikely to disappear completely by anti-inflammatory treatment. The probability of malignant transformation of inflammatory pseudotumor is very low and can be ignored. Therefore, if the patient has no symptoms, the lesions are relatively small, and the morphology has not changed during the follow-up, treatment is not required at this time, and long-term follow-up can be continued. For symptoms such as fever, cough, and expectoration, or if the lesions are large and oppress the surrounding lung tissue, surgical resection is recommended.
When CT images are suspected of malignant tumor, but it is impossible to determine whether it is inflammatory pseudotumor or lung cancer, it is recommended to perform lung puncture or bronchoscopy for biopsy first to confirm the pathology. If a pulmonary pseudotumor is confirmed by pathological examination, as much normal lung tissue as possible should be preserved without lobectomy.