There have been many friends in the background who have left messages for me, asking me to talk about this disease. Well, today we report this disease in the form of several cases, hoping to arouse everyone’s vigilance.
Case 1: Female patient, 36 years old, went to the hospital because of “intermittent limb weakness, palpitations, dizziness for more than 2 years”, and repeated visits, limb weakness, palpitations, dizziness, all of which are It is a relatively common symptom, especially palpitations and dizziness, which generally involve neurology and cardiovascular diseases. Limb weakness is often considered to be a nervous system and endocrine disease, such as whether there is a stroke, whether there is hyperthyroid myopathy, etc.

This patient went to the doctor more often and took a lot of medicines, but the effect was not good. Later, I thought it was hypoglycemia. Low blood sugar can also cause limb weakness, fatigue, palpitations, and dizziness, but the treatment effect of increasing blood sugar is not good. Various inspections were carried out many times and no abnormality was found. Later, a doctor carefully found that the patient was accompanied by emotional tension, insomnia, poor appetite, etc., and suggested referral to a psychologist, who was finally diagnosed as “depression.” After drug treatment, the patient’s symptoms improved significantly, and the symptoms such as palpitations and dizziness gradually disappeared.
Case 2: A 49-year-old male patient presented to the doctor because of “recurrent episodes of epigastric pain, nausea, and anorexia for 1 year”. The patient underwent gastroscopy and was diagnosed with superficial gastritis, but the treatment was effective not good. I still have recurrent epigastric pain, nausea, poor appetite, etc. I also don’t sleep well and lose weight. When I see the doctor, the patient is in a low mood, thinking that his disease can’t be cured, it is an incurable disease, emotional negative. The doctor was more vigilant, and found that the patient’s voice was low, doubting this and suspecting that, and also said that he was terminally ill, living in pain, and life was better than death. The total score measured by the depression scale was 35 points, and depression was considered.
Finally, fluoxetine and lithium carbonate were given, and the condition gradually improved. After 1 month, she recovered and returned to work. The re-measured depression scale was 12 points.
Let me mention to you, the superficial gastritis mentioned by gastroscopy is actually nothing, and most people may have this diagnosis after gastroscopy, so don’t scare yourself.
Case 3: A 29-year-old male patient was diagnosed with allergic dermatitis. He was diagnosed with allergic dermatitis. The effect was not good. Later, it developed into itching of the limbs, chest and abdomen, and sometimes the itching was unbearable. I had to seek medical treatment everywhere, thinking about scabies, diabetic contact dermatitis, eczema, etc. Western medicine and traditional Chinese medicine have looked at it, but there is no improvement.
Later, a doctor was attentive and found that the patient was depressed except for itchy skin, and he had quit his job at home for more than half a year, stayed out of the house, and was unhappy. It was measured by the depression scale. A total score of 32 points was diagnosed as depression. After 2 months of treatment, the patient recovered, and there was no skin itching. It has since been considered that itchy skin is caused by depression itself.
Through the above three cases, you should know that our topic today is depression.
Depression is not far away from us, and there are many people around who have depression. The survey data in 2009 showed that the monthly prevalence of depressive disorder in my country (see clearly, the monthly prevalence) was 2.0%. According to the 2010 WHO survey, the annual prevalence of depressive disorder in developed countries is 5.5% and that in developing countries is 5.9%. In addition, about 70% of depression will relapse, about 20% become chronic refractory patients, and 10% of patients eventually die by suicide.
Many readers on several of my platforms have contacted me, hoping that I will publish some articles about depression. This also proves that depression is not a rare problem. Everyone should be vigilant. When in doubt, always remember to see a doctor.
Dr. Li solemnly tells readers: Depression is a disease, coronary heart disease is a disease, COPD is a disease, hepatitis B is a disease, asthma is a disease, they are all diseases, but depression Symptoms are mental illnesses. Others are physical illnesses and must be treated. Do not feel that mental illness is shameful, inferior, or taboo. Don’t, many mental illnesses are also related to the nervous system, and they all need treatment. of. Ordinary people should not think that depression is scary, and coronary heart disease is not scary. This kind of understanding is also wrong.

I must be frank. Dr. Li has relatively little exposure to depression and rarely encounters such patients in his work. My impression of depression is still in college textbooks and internships in psychiatric hospitals and schizophrenia. It only lasted for 2 weeks, and there is not much awareness. The following sources of data are textbooks and literature
1. Why do I suffer from depression?
Research shows that trauma and adverse life events are significantly associated with onset risk and severity of depression in adults. Stressful life events are also important risk factors.
However, the cause of depressive disorder is unknown, so there is no cure. There are many hypotheses about the etiology, including genetic factors, neurobiological factors, psychosocial factors, etc.
Depression is clustered in families, and the number of parents, siblings, and children of patients with depression is significantly higherIn the general population, some people think that depression is related to genes. But it is generally believed that genes only determine the susceptibility to depression, and the environment is the trigger for depression. In other words, depression is the result of a combination of genes and environment.
What about neurobiology? This is more complicated, mainly caused by the abnormal secretion of some neurotransmitters, and the research is not thorough enough, nor can it be fully explained, it can only be said to be a hypothesis.
Psychosocial factors are very important. The vast majority of depression patients have certain psychosocial factors at the first onset, such as unpleasant events, especially serious life events (such as parental divorce, abuse, etc.), subsequent events, or chronic stressful events (such as marital discord, cold violence, etc.).
In general, the cause of depression is not completely clear, and when it is coming, we cannot predict it, but we must be vigilant and detect it early.
2. What are the symptoms of depression?
Depressed mood, loss of interest, and lack of pleasure are core symptoms of depression.
The so-called low mood is easy to understand, that is, a bad mood, a low mood, or even pessimism and despair, feeling that this is the case in this life, this disease can not be cured, and I have lost my life. Looking forward to it, even looking for short-sightedness.
All of a sudden I don’t like the activities, programs, etc. I liked in the past. For example, I used to like singing and playing the flute, but suddenly I don’t want to open my voice, and the flute is put on the shelf. He sighed and sighed all day long, his brows furrowed, his face full of sadness, and he was silent.
Most patients also suffer from anxiety, irritability, etc.
Slow thinking, conscious brain turning slowly, memory loss, inability to concentrate, feeling pessimistic about everything, this pessimism cannot be faked, it is real. Recalling the past, I will exaggerate some small things and consider them to be unforgivable sins, such as stealing the eraser at the same table, failing the college entrance examination at the same table, and linking these two things, I blame myself. Thinking about the future, I feel that the future is slim, I am a burden, pessimistic, and life is better than death. Severe cases have suicidal behavior.
Reduced verbal actions are an external sign of low mood. The patient is reticent, moves slowly, and has reduced activity. In severe cases, they may be bedridden, not eating or drinking, and lazy to groom. People who usually love cleanliness suddenly become sloppy and do not like to do housework.
The above are typical manifestations of depression and are also well known to the public.
But depression also has somatic symptoms. These somatic symptoms often cause misunderstandings, causing the patient, others, and even doctors to have misunderstandings and make a wrong diagnosis of the disease. For example, the three cases at the beginning of the article are mistaking depression for other diseases.
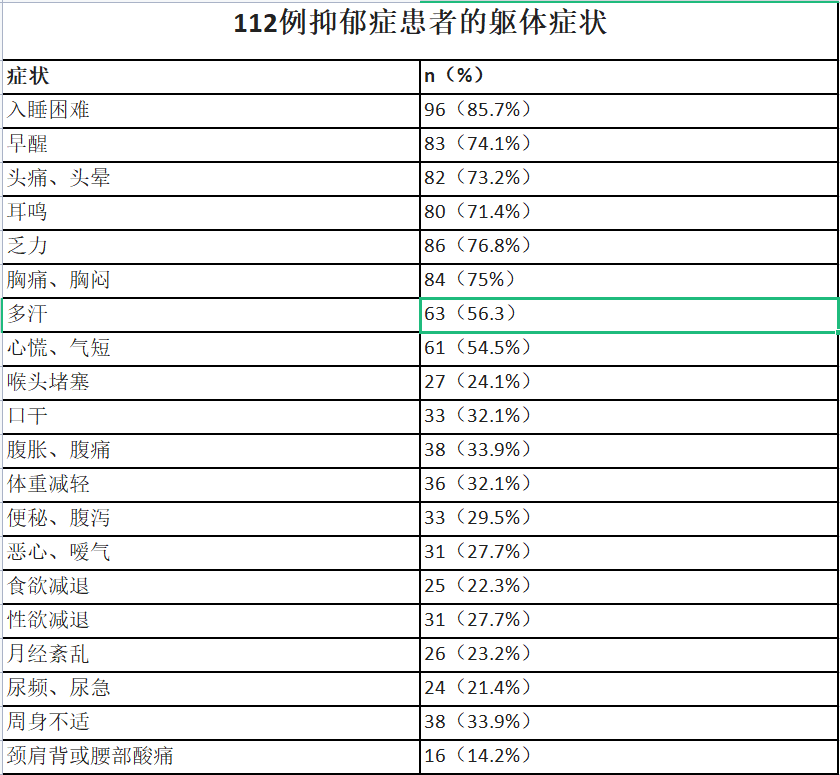
Common physical symptoms include: difficulty sleeping, decreased appetite, weight loss, constipation, decreased libido, amenorrhea, back pain, muscle pain, headache, and more.
I found a study of 112 patients with depression and analyzed their physical symptoms as follows:
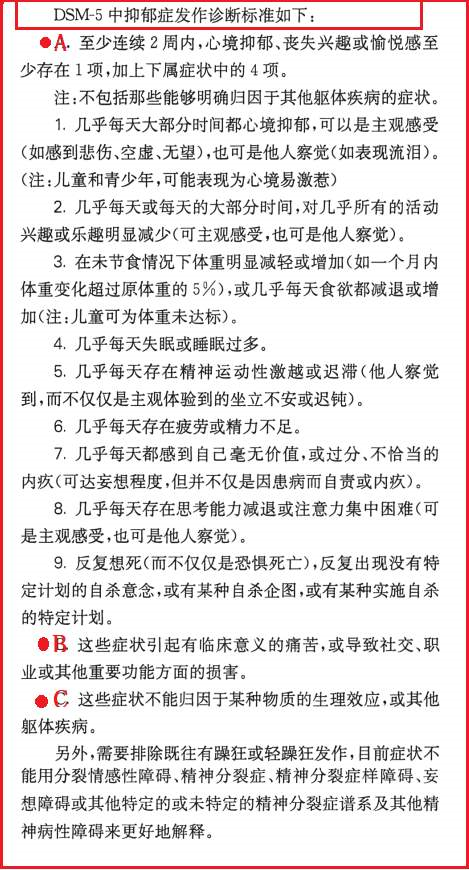
3. How can I tell if I have depression?
Diagnosis of depression is not too difficult, and you should be vigilant when you have the above symptoms. You can look at the table below and meet the ABC to be considered for diagnosis. A may be easier to deal with, the difficulty is in C. Because the diagnosis of depression must first exclude some physical diseases, such as some patients with hypothyroidism will have similar symptoms of depression, but after treatment, hypothyroidism can be recovered, and depression cannot be diagnosed, so the outpatient department of psychology teachers usually check the patient’s thyroid. Function, the purpose is to rule out the influence of hyperthyroidism or hypothyroidism.
Also, hepatolenticular degeneration or other types of hepatitis may present with symptoms similar to depression.
Once you suspect that you may have depression, or someone around you may have this possibility, advise them to seek medical treatment at a professional institution as soon as possible, make a diagnosis of depression as soon as possible, and intervene as soon as possible. Once again, depression is also a disease. Don’t demonize depression. The reason why patients have strange cognitions is because they are sick. Just like schizophrenia, patients are suffering, and drugs can solve the problem, even if not all, but most of them can be solved, which can save lives for patients and their families.
4. How to treat depression?
The goals of treatment for depression are: relief of depressive symptoms (clinical cure) and return of functional levels to pre-morbid states. At present, the whole process of treatment is advocated, that is, acute treatment, consolidation treatment, and maintenance treatment. In other words, do not stop the drug casually.
Why not just stop taking the medicine? Depression requires long-term treatment because of its high recurrence rate and high disability rate. It is necessary to let patients and their families know that they should be prepared for a protracted battle and take long-term medication control. There are too many diseases that cannot be cured. Depression is not alone. Coronary heart disease, asthma, chronic obstructive pulmonary disease, hypertension, hepatitis B, diabetes, most cancers, etc. Which one is curable? Basically, long-term drug control is required.
Drug treatment is the most important method, and there are many kinds of drugs, but the overall efficacy is similar, and the effective rate is 50%-70%. The currently preferred effective antidepressant drugs are as follows:
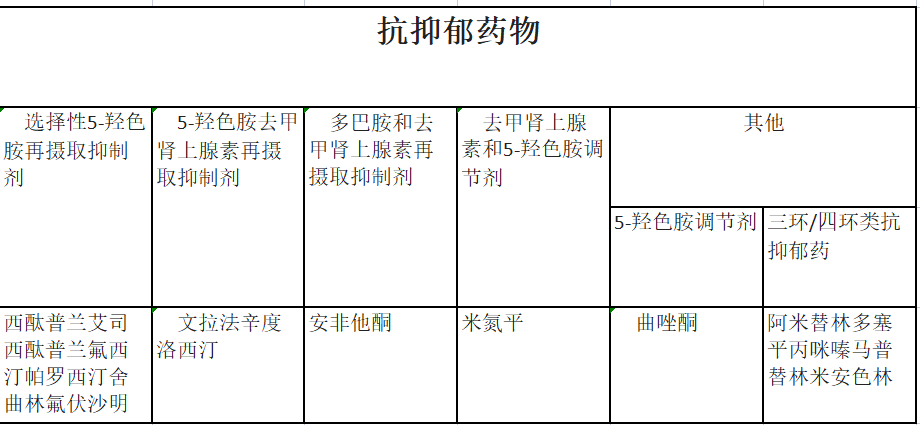
(Chart from: Practical Internal Medicine, 15th Edition)
In addition to medication, there is physical therapy, including modified electroconvulsive therapy, transcranial magnetic stimulation. The effective rate of electroconvulsive therapy is 70%-90%, which is higher than that of antidepressant drugs.
Let’s briefly talk about modified electroconvulsive therapy. The earliest was ordinary electroconvulsive therapy. At the beginning, some doctors found that inducing epilepsy can treat mental disorders and depression. Later, electroconvulsive therapy was developed, which is to let the patient’s brain go through electrical stimulation in a short period of time to induce epilepsy and control. Mental disorders. Everyone must have heard that the patient was given an electric shock, violent convulsions, and then the mental disorder was temporarily controlled. However, electroconvulsive therapy seems too cruel, as if it is punishing the patient, and it is also prone to many complications, and it is even prone to strong muscle contractions that cause fractures.
Now our electroconvulsive therapy is improved, and the patient is given a sedative first (loss of consciousness, no pain), and then a muscle relaxant (to keep the patient’s muscles from cramping) , and then give electrical stimulation. At this time, the patient’s brain will have epilepsy waveforms, but the limbs will not twitch, they feel more comfortable, and their family members will also feel more humane, instead of the horror that requires several people to hold the patient like before. .
But this modified version of electroconvulsive therapy is also risky, because sedatives, muscle relaxants are injected, and the patient loses spontaneous breathing during treatment, which requires an operator (usually He is an anesthesiologist) who pays close attention to the patient’s condition, and gives assisted breathing to maintain the patient’s oxygenation, so that the patient can resume spontaneous breathing smoothly. Now there is an improved version and then upgraded, using a longer-acting muscle relaxant, and then using an anesthesia machine, the patient is safer, and the treatment effect is better, but the action is also very large, every time it is similar to the whole operation. Hemp like that.
In general, improved electroconvulsive therapy is a method, but it is generally used for more severe patients with poor drug treatment effect, and it is not successful in one or two times. It takes several courses of treatment, and it may still relapse later, and it still has to be combined with drug treatment.
5. When can I stop taking the medicine?
As we just said, depression is best controlled with long-term medication. After the acute phase improves, there is also a consolidation phase to prevent relapse. The consolidation period is 4-9 months, and the dose of therapeutic drugs is the same as that in the acute period. After the consolidation phase, enter the maintenance phase of treatment.
In principle, long-term medication is the safest. However, some patients are more ideally controlled, and they are really unwilling to take long-term medication, so can they stop the medication? It is possible to try, but it is risky. If the disease is stable, the drug can be gradually tapered after a period of maintenance. Avoid abrupt discontinuation, and gradually reduce the dose. The first 2 months after drug withdrawal is a high-risk period for relapse, and once relapse occurs, medication should be taken in time. Moreover, patients and their families should be informed that there is a risk of relapse after drug withdrawal, as well as drug withdrawal syndrome.
I hope that all patients with depression can get appropriate treatment. When you have the above conditions, don’t be afraid to avoid doctors. All symptoms are caused by diseases, not real conditions. You think that the future is bleak and that life is better than death. In fact, it is not that life is better than death, but it is caused by disease. Using medicine can improve this situation.
Blessings.