This year’s 5-year-old Kaikai often excretes a small amount of dark red stool when she defeces in kindergarten. The kindergarten teacher suggested that Kaikai’s mother go to the hospital to check her child. Kaikai’s mother felt that the child was so small and lively, able to eat and sleep, so she didn’t take the teacher’s words to heart. One day, when the child was playing in the kindergarten, his stomach hurt badly. Kaikai’s mother hurriedly took the child to the local hospital for examination. Ultrasonography found that the child had “intussusception”, and it was considered “colon polyps secondary to intestinal tract”. Nested“. Kaikai’s mother found Gao Yu, director of the Digestive Endoscopy Center of Shandong Maternal and Child Health Hospital.
Director Gao’s team quickly prepared Kaikai for bowel cleansing. On the second day of admission, the colonoscopy was completed. A 3.5*4.0 piece of 3.5*4.0 was found in the transverse colon near the splenic flexure. cm hemispherical pedunculated polyp, underwent endoscopic polypectomy, and the pathological result was “juvenile polyp“. After three days of postoperative observation, Kaikai recovered and was discharged from the hospital.
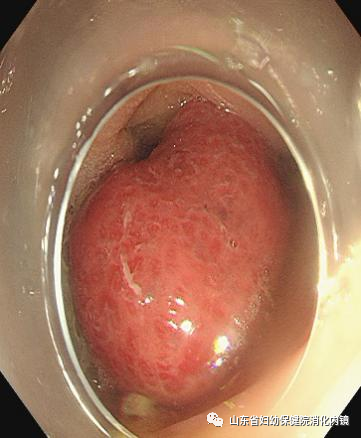
(Endoscopic appearance of polyps)

( polyp removed)
01
What is an intussusception?
Intussusception is when a section of intestinal tube is invaginated into the intestinal lumen to which it is connected, causing obstruction to the passage of the contents of the intestinal lumen, commonly known as “intestinal knots”. This disease is the most common acute abdomen in infants and young children, and the incidence rate is high in my country. The incidence of intussusception in adults is low.

02
What is intussusception?
The intussusception part consists of three layers of intestinal walls: the outer layer is the sheath (outer cylinder), the middle layer is the folded part of the intussusceptible segment (middle cylinder), and the innermost layer is the sleeve The return part (inner cylinder) of the stacked intestine segment, and the front end of the sleeve part is the head. The entrance of the invaginated intestinal segment is the neck, and the mesentery is attached to one side of the intestinal wall, and enters between the middle tube and the inner tube with the intussusception of the intestinal segment.
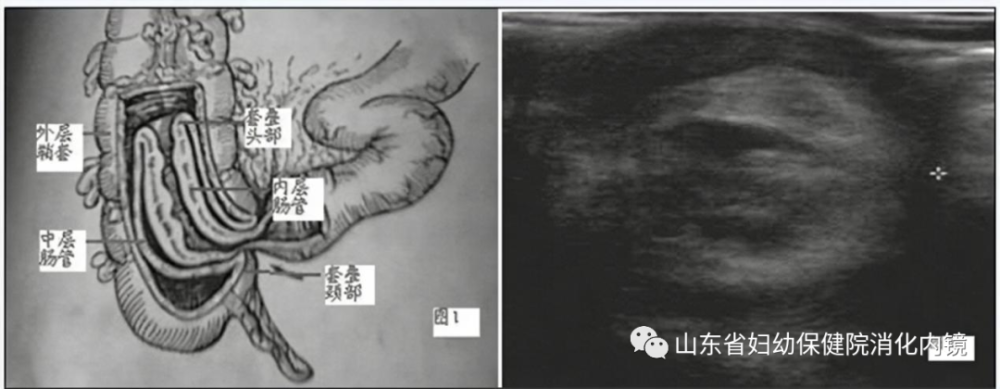
Typical ultrasound findings of intussusception:
1. “Concentric circle sign”: It is characterized by a large ring and a small ring on its cross section, that is, the “concentric circle sign”.
2. “Sleeve sign”: “Sleeve sign” is present on the longitudinal section.
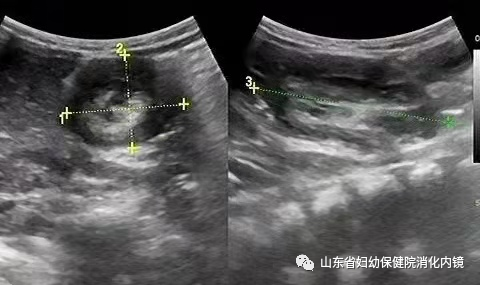
(typical ultrasound appearance of intussusception)
03
Causes of intussusception
1. Primary intussusception: It usually occurs in infants and children, and the cause is unknown. Generally, it is related to changes in diet, the mesentery of the ileocecal region of infants and young children has not been completely fixed, and the degree of activity is relatively large.
2. Secondary intussusception: For intussusception in children >3 years old, the possibility of secondary intussusception should be highly suspected. More common in intestinal duplication malformations, intestinal tumors, intestinal polyps, intestinal infections and so on.
04
Common clinical manifestations of intussusception
Blood in the stool: Usually bloody jam-like stools, but can be fresh bloody or bloody stools.
Abdominal pain: Abdominal pain is usually paroxysmal, lasting about 10-20 minutes each time. This regular abdominal pain is caused by the strong peristaltic wave pushing the invaginated bowel forward, pulling the mesentery, and at the same time, the invagination sheath is strongly contracted.
Abdominal mass: It is usually a sausage-like mass, and the location of the mass changes with different stages of the disease. In the early stage, it is mostly located in the right upper abdomen, and in the late stage, it moves to the left side of the abdomen along the colon, and the farthest into the rectum.
Shandong Maternal and Child Health Hospital Digestive Endoscopy Center once again reminds everyone that if a child has blood in the stool, it should not be underestimated. It is necessary to take the child to the hospital for examination in time to clarify the cause and treat it in time. (Text/Edited by Jia Li/Xu Xiao)