Acute myocardial infarction is the leading cause of sudden death!
In the rescue of acute myocardial infarction, every second counts, so is there any other way to rescue acute myocardial infarction other than stents?

First, in the rescue of acute myocardial infarction, the first is to open blood vessels as quickly as possible
Current guidelines for the diagnosis and treatment of acute myocardial infarction suggest that interventional therapy should be performed first if intervention is possible, and thrombolytic therapy cannot or is unwilling to intervene.
Whether it is interventional therapy or thrombolytic therapy, there is only one purpose, to open blood vessels. Because acute myocardial infarction is a blood clot that blocks the blood vessel. The heart can suddenly stop or ventricular fibrillation at any time, and the myocardium is constantly dying. The more myocardium is necrotic, the greater the risk of sudden death and the greater the risk of heart failure in the future.
Why do guidelines recommend intervening first?

Intervention is simply the method of balloon or stent, which is to use a minimally invasive method to open blood vessels.
Because this method has a clearer effect on opening blood vessels and can save the lives of more myocardial infarction patients, the guidelines recommend immediate intervention.
However, the method of opening blood vessels, in addition to the interventional method of balloon stent, is thrombolysis. Because many hospitals currently do not have the conditions for intervention (no catheterization room, no machine, no interventional doctor), then only the method of thrombolysis can be used.
Thrombolysis is an infusion, but the infusion is not an ordinary liquid, but a thrombolytic drug. Within 3 hours of the onset of acute myocardial infarction, the latest thrombolytic drugs and interventional procedures have basically the same effect of opening blood vessels.
But after 3 hours, the effect of thrombolysis decreased significantly, which is why the guideline recommends intervention first, because most patients with myocardial infarction arrive at the hospital more than 3 hours .
Another reason, even if the thrombolysis is successful, that is, the blood vessels are opened. This kind of blood vessels is opened, only the blood flow is restored, but the plaque of the blood vessels still exists, and the fixed stenosis of the blood vessels still exists. Patients may also experience angina pectoris and even re-thrombosis. Then most patients with successful thrombolysis have to go back to interventional therapy, so it can only be recommended to intervene first.
What is the difference between a balloon and a stent:
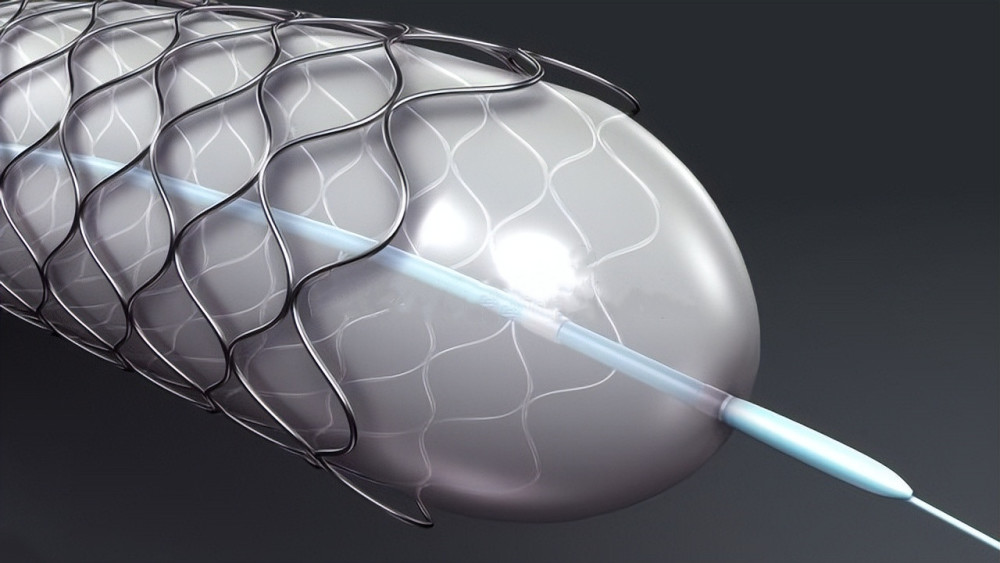
The metal on the outside is the stent, and the inside is the balloon
Balloon expansion must be performed before stenting, and there must be a balloon device in each stent.
It’s just that for some lesions, the doctor will only use balloon expansion according to the specific situation. After expansion, the lumen of the blood vessel can return to normal and the blood flow will be normal. And this part of the lesions is comprehensively judged by the doctor and can be kept in between, then the operation is over.
However, for some lesions, balloon expansion alone cannot solve the problem, and in the end, stents must be implanted after the balloon.
Second, opening the blood vessels is not the whole of the treatment of acute myocardial infarction
The method of intervention (balloon + stent, or balloon) and the method of thrombolytic therapy mentioned above are just methods of opening blood vessels.
But acute myocardial infarction is also coronary heart disease, and it is a special coronary heart disease, so the basis of treatment is almost the same as the treatment of coronary heart disease.

For example:
1. In life: Quit smoking and drinking, don’t stay up late, eat healthy, exercise properly (under the guidance of a doctor, because some people have heart failure, activities should be appropriate) .
2. Regular re-examination: After acute myocardial infarction, one should go to the hospital for re-examination at 1 month, 3 months, half a year, and every year thereafter. Review items include: electrocardiogram, blood (blood routine, liver function, kidney function, muscleAcid kinase, blood sugar, blood lipids, etc.), and a heart ultrasound is reviewed every six months to one year. If symptoms of angina pectoris are present, coronary CT or coronary angiography should be reviewed if necessary.
3. Medication:
Control the three highs, It is generally recommended to control blood pressure below 120/80mmHg, LDL cholesterol below 1.8mmol/L, and heart rate at 60 beats/L cents or so.

Aspirin + statin, This golden combination is the basic treatment for coronary heart disease or myocardial infarction. infarction.
Stent placement requires clopidogrel or ticagrelor for 1 year – 1.5 years.
After myocardial infarction, as long as there is no hypotension or drug allergy, long-term use of pullites, or sartans is recommended; the purpose is to prevent ventricular Expanded, for the prevention or treatment of heart failure.
After myocardial infarction, as long as there are no contraindications to lorol, it is recommended to take lorol for a long time. The purpose is to prevent arrhythmia, to prevent and treat Heart failure.
If myocardial infarction still has angina pectoris, according to the specific situation, review the angiography if necessary; some people need to take drugs to control angina pectoris under the guidance of a doctor, such as diltiazem, nicorandil, trimetah azine etc.
In short, for acute myocardial infarction, stents are indeed the best choice for rescue; but after stenting, it is not the end of treatment, but the beginning of treatment!