*For medical professionals only
Patients with congestive heart failure have reduced renal blood flow and glomerular filtration rate, which may lead to diuretic resistance
A 52-year-old woman presented with dizziness and occasional slurred speech while answering family questions. At first, the family didn’t pay attention, but after 3 days of this phenomenon, she became more and more tired, so she came to the hospital for medical treatment accompanied by her family.

Figure 1 The appearance of a woman holding her forehead and feeling dizzy
Initial Diagnosis
The patient was admitted to the hospital after being examined by the outpatient doctor. The patient’s medical record is shown in the figure below [1].
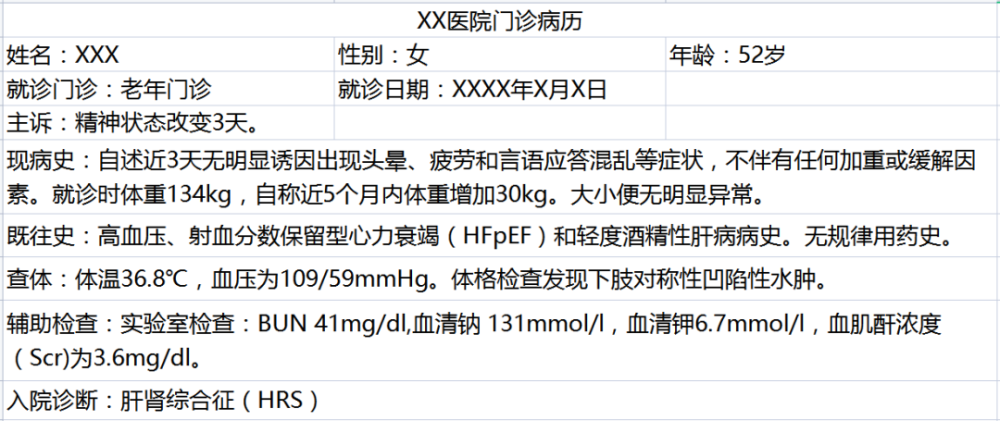
Figure 2 Outpatient medical records
Acute tubular necrosis was ruled out due to lack of specific cause, urinalysis, and significant volume overload. The patient was initially diagnosed with hepatorenal syndrome (HRS), and the outpatient doctor carried out corresponding treatment: intravenous infusion of furosemide + insulin + glucose, human low-salt albumin, midodrine hydrochloride and Octreotide acetate therapy. The treatment was effective initially, and the hyperkalemia was successfully corrected, but the patient’s edema symptoms did not improve. On the third day of the patient’s admission, her doctor in bed sought the help of a nephrologist at the hospital to explore the patient’s cause.
Transfer to Nephrology, patient worsens
When the nephrologist arrived in a hurry, the patient was found to be in a dire state.
Physical examination showed dilated jugular veins >5-8cm H2O, decreased breath sounds at the base of the lungs, and pitting edema (++) in the lower extremities to the lower abdomen.
Laboratory values include hemoglobin 8.7g/dl, platelet count 109000/l, serum sodium 140mmol/L, serum potassium 3.8mmol/L, serum chloride 106mmol/L /L, total serum CO223 mmol/L, BUN 47mg/dl, Scr 3.47mg/dl and proBNP 1170pg/ml, blood glucose, calcium and liver enzymes were normal, but plasma albumin decreased by 2.5g/dl.
urinalysis showed a specific gravity of 1.017 and no proteinuria or casts. Urine sodium and chloride concentrations
Chest X-ray showed signs of pulmonary edema.
A echocardiogram 2 weeks earlier showed a preserved ejection fraction of 60%-65% and diastolic dysfunction.
Abdominal ultrasonography was negative for ascites.
After comprehensive consideration, the patient was diagnosed with heart failure with preserved ejection fraction (HFpEF) worsening, bedside specialist consultation, A treatment plan was customized for her immediately.
1-5 days in hospital
Diuretic therapy was intensified with furosemide 80 mg + hydrochlorothiazide 250 mg IV twice daily. The patient’s urine output (UV) increased moderately from 350ml to 550ml.
Diuretic escalation to continuous IV furosemide (20mg/h) + IV bolus hydrochlorothiazide (500mg twice daily), but this failed to Made UV > 1500ml or FENa > 2% and did not improve the patient’s symptoms or change their Scr (as shown in Figure 3).
Diuretic therapy was blocked again, and the specialist decided to further change the dosing regimen.
Day 6 in hospital
During stable diuretic therapy, hydralazine (10 mg tid, orally) was added. Within 24 hours, the patient’s Scr dropped to the lowest point since admission, while UV and FENa doubled. Since then, the patient’s clinical symptoms and various test indicators have gradually improved.
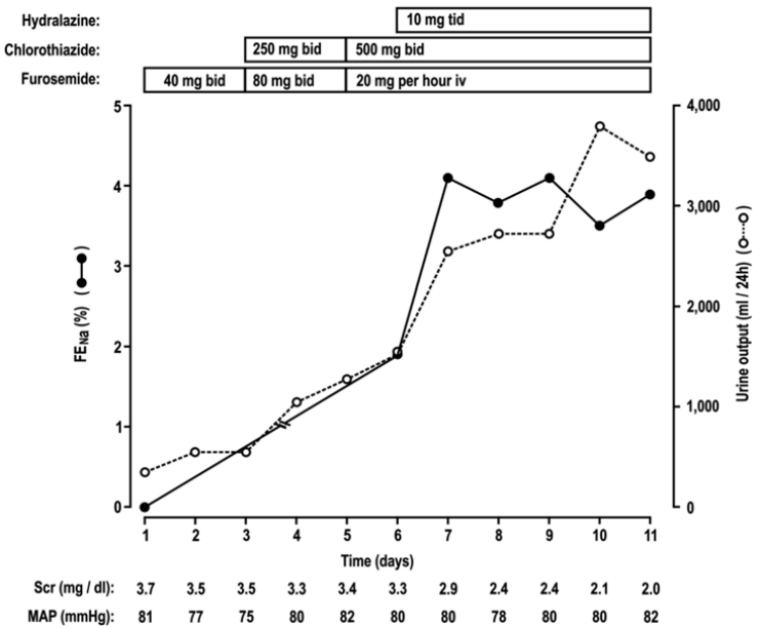
Figure 3. Hydralazine in patients resistant to loop diuretics + thiazidesDiuretic and natriuretic responses of pyridazine. Day 1 is the first day of the nephrology consultation. Abbreviations: FENa, fractional sodium excretion; Scr, serum creatinine; MAP, mean arterial pressure; bid, twice a day; tid, three times a day.
Hospital Day 11
The patient’s clinical status improved sufficiently with furosemide (80 mg twice daily) + spironolactone (200 mg once daily) + hydralazine (20 mg daily) 3 times)‘s oral regimen.
During the 19-day hospital stay, the patient lost 23 kg of body weight, his Scr improved to 1.3 mg/dl, and he was ready for discharge.
The patient was followed up 3 months later. The patient insisted on taking furosemide 80mg and spironolactone 200mg twice a day, the symptoms were controlled, and the weight lost 10kg again.
This woman’s treatment is reassuring, but the doctor’s review of the treatment has not stopped.
Aetiology is suspicious
Analysis of the cases shows that the patient has a complex and uncontrolled condition in the past, and the conventional treatment plan has little effect after coming to the hospital. Expert consultation and discussion concluded that many patients with congestive heart failure have reduced renal blood flow and glomerular filtration rate, which may lead to diuretic resistance, and this is the difficulty of this treatment.
This introduces a concept, what is diuretic resistance?
A review lists some definitions that are clinically applicable, but not yet uniformly recognized by clinicians: patients with persistent edema with more than 80 mg of furosemide per day; sodium excretion as a proportion of load The empirical view is that persistence of symptoms of hyperemia and edema following the use of diuretics, so-called diuretic resistance[2].
After starting the application of diuretics, the patient’s body weight and the amount of sodium in the body decreased, but the balance of sodium intake and excretion was reached very quickly. This physiological antidiuretic effect is the body’s Protection against excessive loss of water and salt. If this balance occurs earlier than the therapeutic target, diuretic resistance occurs.
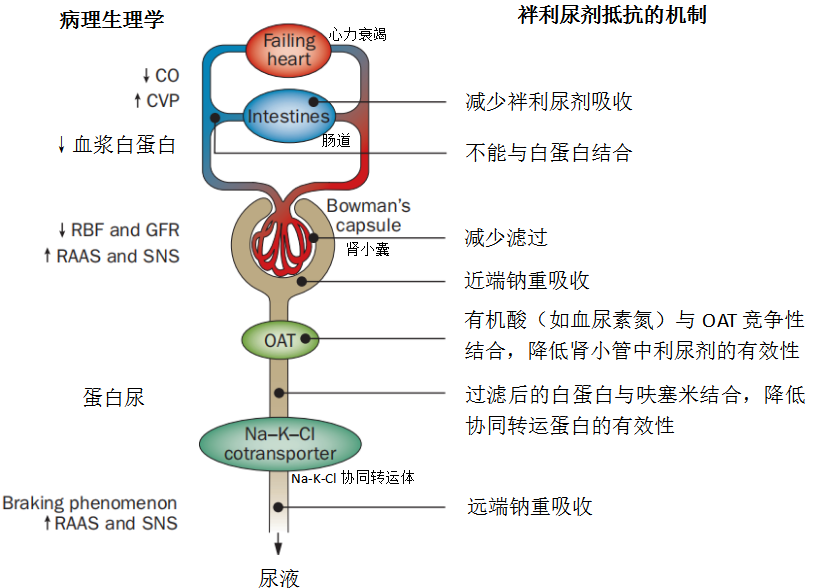
Figure 4 Mechanisms of loop diuretic resistance. Patients who are resistant to loop diuretics may have decreased intestinal absorption, decreased filtration, or increased renal proximal or distal sodium reabsorption, or decreased renal tubular availability. Abbreviations: CO, cardiac output; CVP, central venous pressure; GFR, glomerular filtration rate; OAT, organic anion transporter; RAAS, renin-angiotensin-aldosterone system; RBF, renal blood flow; SNS, Sympathetic nervous system.
How to deal with diuretic resistance in the nephrology department?
The use of diuretics in the nephrology department mainly focuses on nephrotic syndrome and chronic renal failure. The dosage forms of the drugs are mainly loop diuretics. The main reasons for the occurrence of diuretic resistance are: 1) In patients with chronic kidney disease, the damage of renal structure, glomerular sclerosis, and tubulointerstitial atrophy, etc., cause the loss of the target of diuretics. 2) In addition, the blood supply to the nephron decreases, and the dose of the drug in the blood to reach the target also decreases.
The main approaches to diuretic resistance are as follows:
1. Basic treatment: correct hypoalbuminemia, replenish blood volume, treat primary disease, limit salt;
2. Discontinue related drugs;
3. Correct acid-base balance disorder;
4. Correct hyponatremia;
5. Increase the dose of diuretics;
6. Continuous intravenous infusion of diuretics;
7. Combination medication: thiazides, potassium-sparing agents, and loop diuretics.
References:
[2]ter Maaten JM, Valente MA, Damman K, Hillege Hl, Navis G, Voors AA. Diuretic response in acute heart failure-pathophysiology, evaluation, and therapy. Nat Rev Cardiol. 2015;12(3):184-192. doi:10.1038/nrcardio.2014.215
Source of this article: Medical Nephrology Channel
The author of this article: Wang Dabao
Review expert: Prof. Li Qing
Editor in charge: Yuan Xueqing, Zhang Li
Copyright Notice