WuXi AppTec Content Team Editor
Previous studies have shown that about 75% to 90% of gastric adenocarcinomas are associated with Helicobacter pylori (Hp) infection. In addition, about 5% to 10% of gastric adenocarcinomas are associated with Epstein-Barr virus infection. Although nearly 50% of the global population is infected with H. pylori,only 1%-3% of the population will eventually develop into gastric adenocarcinoma due to the combined effects of H. pylori strains, host susceptibility and chronic inflammatory response.
Recently, Nature Reviews Gastroenterology & Hepatology, a sub-journal of “Nature”, published an important review, describing in detail the important influence of Hp in the formation of gastric adenocarcinoma. The paper emphasizes that early detection and eradication of H. pylori infection is crucial for preventing chronic gastritis from developing into gastric adenocarcinoma.
Furthermore, given that host lesions may already have immunosuppressive features years before gastric adenocarcinoma develops, it is useful to identify the process of gastric atrophy to gastric metaplasia Changes in related markers in the gastrointestinal tract may help us improve the prevention and treatment of gastric adenocarcinoma!
Screenshot source: Nature Reviews Gastroenterology & Hepatology
Major risk factors for gastric adenocarcinoma
Globally, nearly 60% of gastric cancer patients are in East Asia, and nearly half of them are in China. Recent studies have confirmed that Hp infection is a strong correlative factor for both non-cardia gastric cancer (including gastric adenocarcinoma) and cardia gastric cancer. In addition, other environmental risk factors for gastric adenocarcinoma include a high-salt diet as well as nitrate exposure. Genetic studies have shown that about 50% of gastric adenocarcinomas are chromosomally unstable gastric adenocarcinomas, and 21% of gastric adenocarcinomas are highly microsatellite unstable (MSI-H) gastric adenocarcinomas.
The vast majority of Hp-infected patients have no obvious symptoms, and at least 20% of the infected people are difficult to eradicate Hp infection with antibiotics due to bacterial resistance and lack of compliance with treatment. The paper emphasizes that under the combined effect of multiple risk factors, nearly 20% of H. pylori infection may develop serious complications (including gastric atrophy, gastric metaplasia, and gastric adenocarcinoma).
Specifically, these factors include:
Environmental factors: such as smoking or tobacco exposure;
Dietary factors: such as higher intake of smoked foods, higher intake of high nitrate foods, high salt diet;
Host susceptibility: Such as genetic variation (including IL-1β, TNF-α and other cytokine gene polymorphisms), iron deficiency, type O blood.
How does Hp drive gastric adenocarcinoma?
About 75%~90% of gastric adenocarcinoma patients show positive serum Hp. Previous studies have shown that Hp infection is associated with persistent immune infiltration (chronic gastritis), and the changes in the immune microenvironment caused by Hp infection (changes the host’s innate immunity, adaptive immunity builds an immunosuppressive environment), It plays an important role in the development of chronic gastritis into gastric adenocarcinoma.
In addition, Hp can also induce the occurrence of related pathological events by regulating vacuolar toxin-related factor A (VacA) and cytotoxin-related factor A (CagA).
Similar to many other solid tumors that originate from epithelial cells, different types of cells in the supporting structures surrounding the gastric tumor can act as initiators, promoters, and promoters to play a variety of roles in its growth. These different types of supporting cells include stromal cells, neuronal cells, endothelial cells, and a large number of immune cells.
The paper emphasizes that it is still unclear which immune cells are involved in the transformation of normal gastric epithelial cells into metaplasia and dysplasia in Hp-related gastric cancer.
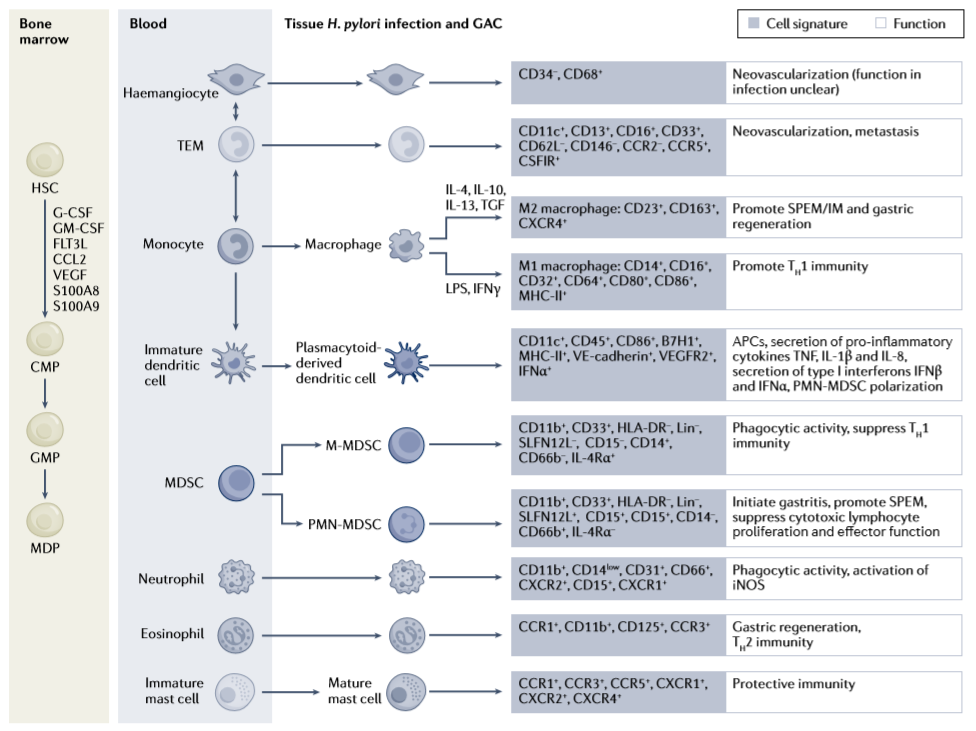
▲Types of immune cells recruited by Hp infection in gastric lesions (Image source: Reference[1])
Hp can be found in different stages of disease progression in patients with gastric adenocarcinoma. In addition to H. pylori, studies have shown that the presence of Prevotella, Streptococcus, Pseudomonas, Sphingomonas, Bacillus and Acinetobacter can also be found in the normal mucosa adjacent to gastric tumors.
In addition, animal studies have demonstrated that Acinetobacter can induce gastritis and induce a TH1-type immune response, and Bacteroides and Haemophilus-related markers are also present in the blood circulation of patients with gastric adenocarcinoma increase in material levels.
Therefore,Although Hp may mediate the initial process of gastric adenocarcinoma, after gastric mucosal atrophy, HpThe role of , other bacteria and immune cells in the development of gastric metaplasia and gastric adenocarcinoma remains to be further explored.
What does early detection and eradication of Hp mean?
Persistence of chronic gastritis can promote gastric parietal cell apoptosis and cause chronic atrophic gastritis. The time from H. pylori infection to serious complications, such as gastric atrophy, gastric metaplasia and even gastric adenocarcinoma, can take months or years. During this period, the gradual reduction of oxyntic parietal cells reduces gastric acid levels and affects the composition of gastric microbes.
Although only a small percentage of people with Hp infection develop clinically significant complications. However, based on the fact that H. pylori infection plays a very critical role in driving the occurrence of gastric adenocarcinoma, early detection, eradication and even prevention of H. pylori infection are very important.
Key nodes in the development of gastric adenocarcinoma
Because tumor neoantigen expression in EBV-positive and MSI-H gastric adenocarcinomas predisposes them to a higher degree of inflammation (ie, “hot tumors”), more It is easy to produce effects under chemotherapy combined with immunotherapy.
In contrast, most subtypes of gastric adenocarcinoma, such as diffuse gastric adenocarcinoma with genetic variation and Hp infection-driven intestinal adenocarcinoma, are immunologically In terms of “cold tumor”. Hp may contain immunomodulatory sequences that promote immunosuppression by inducing Treg cells. In addition, Hp infection-related gastric adenocarcinoma may have an immune escape mechanism, so anti-tumor immunotherapy obviously cannot work.
The paper points out that metaplasia of gastric epithelial cells (including extent and type) is a key node in the development of gastric adenocarcinoma.
Since an immunosuppressive environment in the stomach may already exist years before the diagnosis of gastric adenocarcinoma, a more in-depth study of the inhibitory factors of the immune response during H. pylori infection and exploration of gastric Molecular changes in atrophy at the critical juncture in the transformation of gastric mucosal metaplasia may help us develop biomarkers for early detection of epithelial changes and improve the treatment of gastric adenocarcinoma.
In addition, on this basis, the possible risk factors of the host can be identified. In the future, we can predict which individuals have a higher risk of complications and effectively prevent gastritis from developing into gastric adenocarcinoma.