*For medical professionals only

The patient had repeated chest pains and underwent four coronary angiograms. The culprit was…
It was another night shift. The phone at the nurse’s station rang at night. It was the emergency department calling, and a familiar voice rang in my ear: “Is there a bed? Take a patient, and his vital signs are stable. , I had a stent before, and I had chest pain for 1 day.
“Oh, come on.”
So the nurse makes the bed, prepares the infusion pump, and is ready.
Acute Coronary Syndrome is the most common condition on the cardiologist’s watch, business as usual.
“Chuck cluck…” The rescue bed arrived as promised with the elevator bell. I picked up the stethoscope and rushed to the patient surrounded by nurses and family members. I saw her lying on the hospital bed with brows furrowed. The family members next to her looked anxious and did not care to wipe the sweat off her face. She was carrying a stack of medical information.
Female, 49 years old, with a history of hypertension for 10 years, no history of diabetes, tobacco and alcohol, perimenopausal, her father and brother suffered from hypertension, coronary heart disease, and the father’s history of sudden cardiac death, There are risk factors for coronary heart disease.
5 years ago, I developed episodic chest pain with left arm numbness, lasting 4-5 minutes each time. Coronary angiography was performed in our hospital at that time, which showed proximal lumen of the anterior descending artery. Irregularity, near-middle myocardial bridge, no obvious stenosis and blockage of circumflex artery and right coronary. The chest pain was controlled after drug treatment.
1 week ago, the chest pain recurred, the nature was the same as before, the pain was aggravated, the duration was prolonged, and the sweating lasted for 30 minutes. Coronary angiography was performed in a local hospital, and the results showed: No stenosis in the left main trunk, 40% stenosis in the proximal segment of the anterior descending artery, 50% stenosis in the middle segment, 30% stenosis in the proximal segment of the circumflex artery, 95% stenosis in the distal segment, right coronary artery stenosis 40% stenosis in the middle. A stent was implanted in the distal segment of the circumflex branch. After the operation, anti-platelet, lipid-regulating, vasodilatory, and ventricular rate control drugs were regularly administered orally. However, the chest pain problem was not resolved after stent implantation.
One day ago, the patient had chest pain again, accompanied by numbness and sweating of the left arm, and repeated attacks, lasting 20-30 minutes. Chest pain has eased.
Emergency ECG: ST-segment depression in leads V3-6 in sinus rhythm
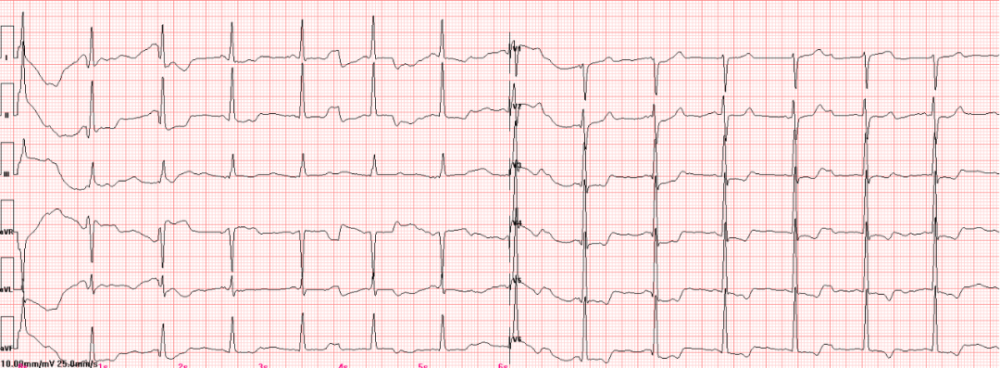
Figure 1 Emergency ECG
Physical examination: body temperature 36.5°C, pulse 70 beats/min, respiration 22 beats/min, blood pressure 190/107mmHg, no positive signs found in cardiopulmonary abdominal nervous system examination.
After inquiring about the medical history, writing the medical records, and issuing the doctor’s order, the urgent test results will be reported: myocardial injury markers, blood routine + C-reactive protein (CRP), D-dimer, Brain natriuretic peptide (BNP), coagulation routine, liver and kidney function and other results were not abnormal.
The patient’s electrocardiogram showed myocardial ischemia, with chest pain symptoms, and a history of percutaneous coronary intervention (PCI) 1 week ago. Arrhythmia, aortic dissection, pulmonary embolism, acute After pericarditis, is this an out-of-hospital patient with post-PCI chest pain? PCI-related ischemia or incomplete revascularization? Or clopidogrel resistance?
Just as I was thinking about the cause of the chest pain, the patient had another episode of chest pain. At this time, it was 0:00, and the “sit-up” mode of my duty was officially started (meaning that the doctor on duty at night lay down a little, about to get up).
The patient had recurrent chest pain 6 times from midnight to early morning, and the ECG still showed mild ST segment depression in the lateral leads during each chest pain attack, which could be relieved by nitroglycerin. After the chest pain was relieved, the ECG ST segment After returning to baseline, diltiazem and tirofiban were given intensive antiischemic therapy.
Contact the surgeon early the next morning to prepare the patient for coronary angiography as quickly as possible.
Angiography results showed: There was no obvious stenosis of the left main trunk, 50% stenosis in the proximal segment of the anterior descending artery, 40%-50% stenosis in the middle segment, and anterior blood flow TIMI III The proximal segment of the circumflex artery is 30%-40% stenotic, the distal stent is unobstructed, and the anterior blood flow is TIMI grade III; the middle right coronary stenosis is 40%-50%, and the anterior blood flow is TIMI grade III.
The stent is unobstructed and there is no obvious residual coronary stenosis. Are you lonely in a hurry? What explains the recurring chest pains?
In view of the patient’s age, considering the causes of perimenopausal female hormone and autonomic nerve dysfunction, and coronary microvascular disease, oral nicorandil was prescribed to improve microcirculation. For the next 3 days, the patient’s chest pain really didn’t come back, and we were relieved. At the same time, the results of the thromboelastography experiment reported: the inhibition rate of clopidogrel against platelet adenosine diphosphate (ADP) was 14% (insensitive), and the inhibition rate of arachidonic acid (AA) was 100% (obvious inhibition). Not at ease, I replaced clopidogrel with ticagrelor.
3 days later, the patient complained of chest pain again. At this time, the ST segment in lead II of the ECG monitoring was significantly depressed. Why is there such a significant change in lead II when the right coronary and gynae are unobstructed? ?
In hindsight, it turns out that it was justThe tip of the iceberg of truth.
In the early morning of the next day, it was another shift night. The patient again suffered sudden severe chest pain and palpitations. ECG monitoring showed ventricular tachycardia, sweating, irritability, and sudden loss of consciousness. , limb convulsions, immediately give electric defibrillation rescue, after the patient regained consciousness. Then the sly killer finally showed his tail. A few minutes later, the patient had chest pain and sweating again. At this time, the ECG captured the ST segment elevation in the anterior leads, and the ST segment fell back 2 minutes later, and the pain was relieved.
Fig.2 ST segment depression in lead II of ECG monitoring
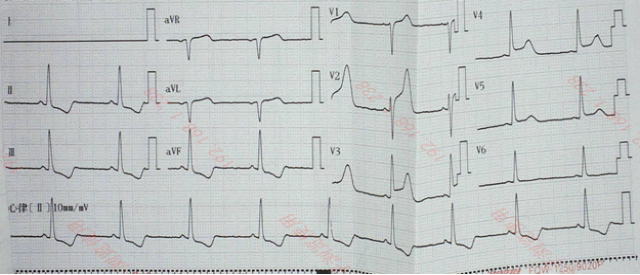
Fig.3 ST-segment elevation in anterior leads of chest pain attack
Patient with chest pain and ventricular tachycardia considered severe anterior descending vasospasm ischemia. According to the guidelines, diltiazem for antispasmodic, atorvastatin for intensive lipid-lowering, isonitrogen Sorbitate to prevent cramps, stop metoprolol. The patient finally did not have chest pain and ventricular fibrillation again after full treatment such as spasmolysis, lipid regulation and coronary expansion, and was discharged from the hospital 7 days later. Recalling the thrilling scene on duty, I can’t help but take a deep breath.
But who would have thought that 3 days later, the patient was admitted to the hospital with chest pains again, and the emergency ambulance saw this patient again. Afterwards, the patient had repeated chest pains of severe nature, and soon received the laboratory critical values, creatine kinase isoenzyme 9.68ng/mL, myoglobin 10.37ng/mL, troponin I 1.733ng/mL, this time a solid myocardial infarction !
ECG monitoring showed significant ST-segment depression in lead II, ST-segment elevation in anterior leads, and short burst ventricular tachycardia. The patient has drug-resistant fatal coronary spasm, and if necessary, the descending stent is implanted before coronary angiography to reduce the risk of sudden death.
For family members who have undergone angiography for three times, angiographic stents are not unfamiliar, but the risk of sudden death on the operating table is extremely high, and no one can be sure whether the spasm blood vessels can be found this time. Stent implantation may have poor efficacy or even ineffectiveness. Will it return empty-handed like the previous three angiography?
At this time, the frequent short burst ventricular tachycardia alarm of the patient’s ECG monitoring is like the knock on the doctor’s heart before death breaks the door. The situation is extremely urgent. After intense discussions and full communication with family members, doctors and patients decided to unite the front and take the stage immediately.
The results of angiography made the surgeon nervous: 99% stenosis in the proximal segment of the anterior descending artery!
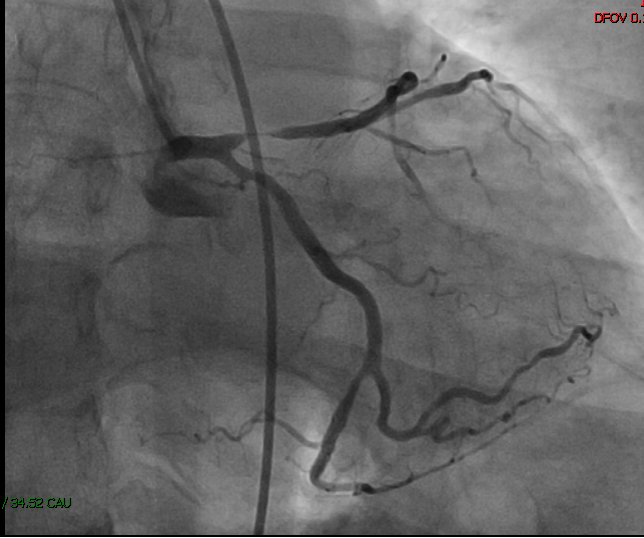
Figure 4 Spastic 99% stenosis of proximal anterior descending artery
A real life on the line! Intracoronary nitroglycerin was administered immediately and blood flow was restored.
After four imaging sessions, coronary spasm, the sinister and cunning murderer, was finally caught.
The disease of spasticity is choking the patient’s life, and delusions make the patient submit. At this time, if you follow the guidelines and recommend simple conservative treatment with drugs, it is tantamount to disarming the doctor and putting the patient on the edge of the cliff. .
In the face of a dead end, we must have the courage to open up a way to survive, and learn from the domestic and foreign case evidence of stent treatment of coronary spasm, so we sent a stent along the guide wire at the most severe spasm in the proximal part of the anterior descending artery. , seeing the smooth blood flow in the stent immediately after the balloon expansion, as if seeing the collapse of the enemy, spasm, after our throat was choked by us, the hanging heart finally fell.
Continued to strengthen antispasmodic, lipid-lowering, and coronary expansion after the operation. There was no chest pain or arrhythmia during the 2-year follow-up after discharge, and the clinical symptoms were completely relieved.
This rescue experience gave me a lot of insight: difficulties and setbacks are always inevitable on the way of clinical diagnosis and treatment. Medical practitioners should not forget their original aspirations, should not give up easily, and should be brave Yes, fulfill the mission of curing diseases and saving people; in the process of clinical exploration, we must follow the authority but not stick to it; in the current tense medical environment, full knowledge and communication are the keys to obtaining the understanding and cooperation of patients and eliminating the gap between doctors and patients. Still an ally in the trenches.
Sometimes a disease is like a cunning rabbit, constantly hiding and creating illusions, just like the “three caves of a cunning rabbit”, always making doctors and patients rush around, but no matter how cunning the prey is, the hunter is no match for it , The realm of clinical exploration and analysis of difficult problems is “there is no way to doubt the mountains and rivers, and there is another village in the dark.” Today’s case is shared here. Colleagues are welcome to share their experience and experience on the way of practicing medicine in the comment area. See you next time.
This article was first published: Cardiovascular Channel of the Medical Community
The author of this article: Medical Sea Picking
Review of this article: Jiehui Zhao
Editor in charge: Yuan Xueqing, Zhang Li
Copyright Notice