Nowadays, people are paying more and more attention to their health, and many people find that the word “polyp” appears on the medical report: Intestinal polyps, gallbladder polyps, cervical polyps, endometrium Polyps…
At first glance, it is inevitable to be nervous and worried. What is this “polyp”? Does it have anything to do with cancer? Does it have to be surgery?
Today, let’s get closer to the true face of the “polyp” of Mount Lu!
In addition to the surface of the human body relative to the outside world – the skin, there is also an inner surface – the mucous membrane inside the organs.
Polyps refer to the growths on the surface of the human mucosa, which can appear up to the nasal cavity, vocal cords, down to the rectum and cervix. Name the part where it grows.
Polyps themselves are benign lesions, but some of them may become cancerous, so Which polyps can be reassured and which ones should be paid attention to?
 Image source: Zhanku Hailuo
Image source: Zhanku Hailuo
1
Intestinal polyps: some are “ticking time bombs”
Intestinal polyps are not necessarily cancerous.
Intestinal polyps are relatively common diseases. They are abnormal growth tissues protruding from the surface of the intestinal mucosa. Before there is no pathological classification, they are collectively referred to as “polyps”.
Whether intestinal polyps are at risk of cancerous development, and whether resection is beneficial or not, depends on the connection method, size, extent, number, morphology, pathological type, and family history of intestinal tumors etc. [1,2].
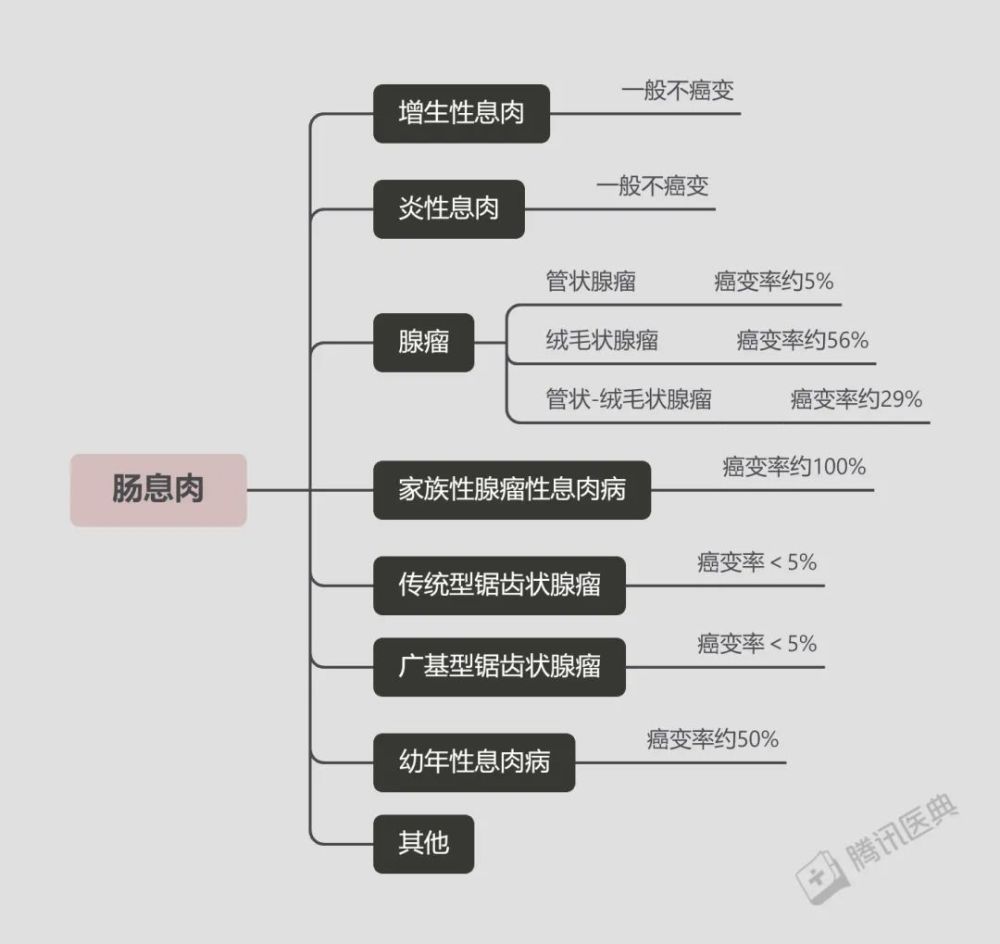
For example, inflammatory polyps, and hyperplastic polyps belong to the same non-neoplastic polyps. They are usually caused by inflammation to stimulate the mucosa and have little tendency to become malignant [3].
usually treat primary bowel disease (eg, ulcerative colitis, Crohn’s disease), periodic review, not Must be removed.
Neoplastic polyps include adenomatous polyps and serrated polyps[3].
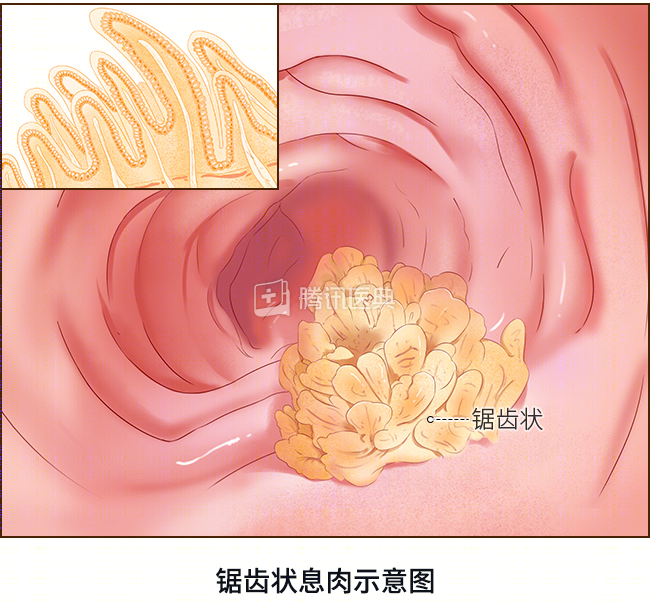
They are divided into many types. In short, The larger the diameter and the more fluff contained in it, the higher the risk of malignant transformation[4], generally need resection.

Regardless of the type of polyp, it is recommended that you go to the gastroenterology department in time, choose the appropriate treatment, and review it according to the doctor’s order.
If you’ve recently been diagnosed with the aforementioned neoplastic bowel polyps, don’t worry too much, because it’s usually a while before the cancer evolves.
It is estimated that it takes 5-10 years for most macroscopic polyps to become cancerous[3].
However, the sooner it is detected and treated aggressively, the better chance it has to nip cancer in its cradle.
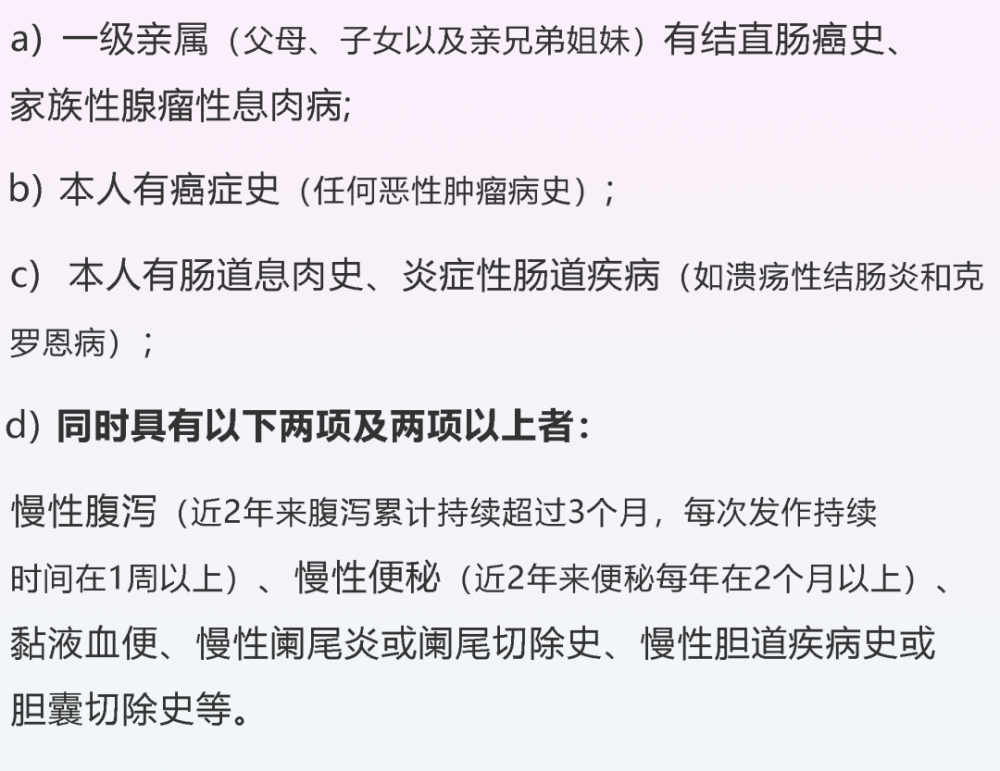
Of course, this requires timely screening colonoscopy, especially in high-risk groups.
Because relatively speaking, this group of people may have polyps in their intestines at a younger age.
It is recommended for people over 45 years of age to do it once, even if there is no discomfort, The frequency of follow-up examinations is determined according to the examination results and relevant medical history[5].
High-risk groups should start screening earlier and increase the frequency of screening as recommended by their doctor.
2
Gallbladder polyps: the vast majority are benign
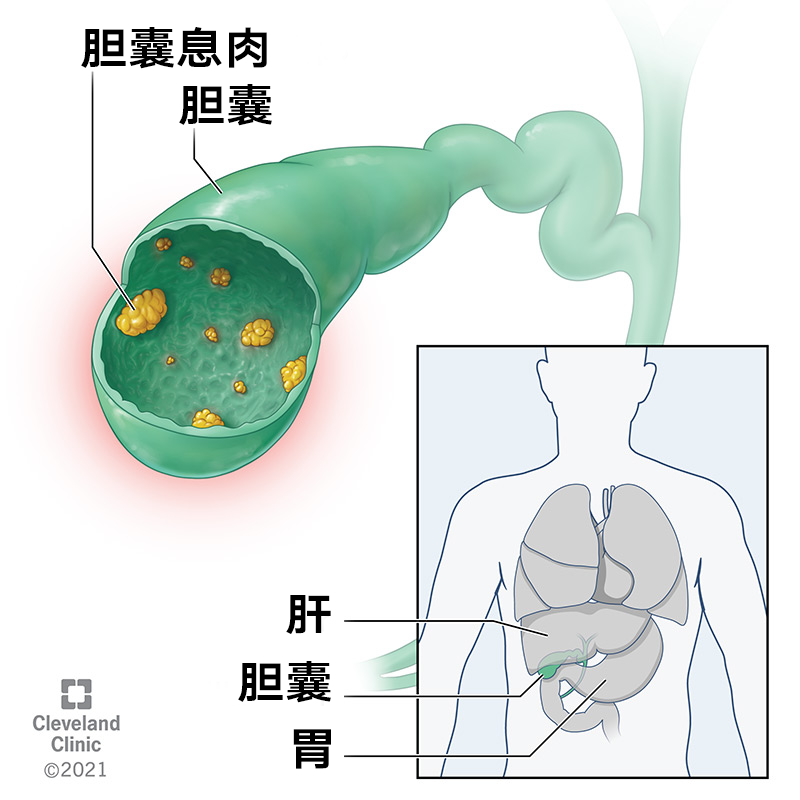
(Source: Cleveland Clinic)
The vast majority of gallbladder polyps are benign.
Gallbladder polyps are relatively common, and the incidence in Chinese is about 6.9%-9.6%, of which only about 5% are malignant polyps [9,10].
About 60% of gallbladder polyps are cholesterol polyps[10], which are mainly caused by excessive cholesterol phagocytosis by phagocytes of the gallbladder mucosa, which is closely related to blood lipid levels. The relationship with a high-cholesterol diet is unclear.
Inflammatory polyps, associated with tissue proliferation caused by inflammatory stimuli (eg, cholecystitis, gallstones).
Cholesterol polyps and inflammatory polyps are generally not malignant, and regular reexamination is enough. More attention should be paid to adenomatous polyps and gallbladder adenomyosis (controversial) ), may have cancer risk [11,12].
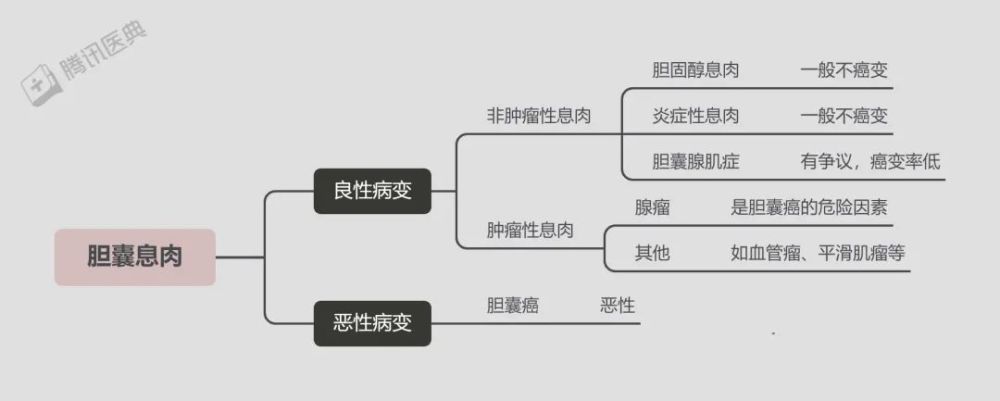
Comparatively speaking, large size, fast growth rate, wide base, combined gallstones, older patient (>50 years old), daring Gallbladder polyps with obvious symptoms such as colic are at greater risk, and doctors may recommend surgical intervention to prevent polyps from becoming cancerous and relieve clinical symptoms [13].
3
Cervical polyps: small polyps don’t worry
The vast majority of cervical polyps are caused by chronic inflammation and long-term stimulation, most of them have no obvious symptoms, and a few have abnormal leucorrhea, irregular vaginal bleeding, bleeding after sexual intercourse, dripping menstruation, etc. [14,15].
The vast majority of cervical polyps are benign, and only about 0.2%-1.5% are at risk of malignant transformation[16].
Asymptomatic cervical polyps do not necessarily need to be treated, but if the polyp is too large (basal diameter ≥ 1cm), has obvious symptoms, and has fertility needs, it can be treated Surgical resection, and pathological examination to rule out the possibility of malignant transformation [17].
 Image source: Zhanku Hailuo
Image source: Zhanku Hailuo
4
Endometrial polyps: some go away on their own
Endometrial polyps are a common gynecological disease caused by excessive endometrial hyperplasia. The etiology and pathogenesis are still unclear. They can be found in all age groups, the most common in 40-50 between the ages.
Endometrial polyps smaller than 10 mm, about 25% may resolve spontaneously[18], and the smaller the polyp, the easier it is to disappear, possibly after several menstrual cramps Disappeared with the peeling of the intima.
Most endometrial polyps are benign, and only about 0 to 12.9 percent of endometrial polyps have the potential to become malignant [21,22].
In general, premenopausal endometrial polyps have a lower risk of malignancy, and postmenopausal polyps, especially those with vaginal bleeding, have a higher risk of malignancy.
In addition, old age, obesity, hypertension, polyp size (>15mm), hormone replacement therapy, etc. are also high risk factors, so , treatment is generally recommended [21,22].
Now we know that not all polyps become cancerous.
Regular physical examination, scientific treatment of polyps, and following the advice of specialists are the best health protection for us!
 Image source: Zhanku Hailuo
Image source: Zhanku Hailuo
Reviewer
Gao Pengji| Chief Physician of General Surgery, Beijing Jishuitan Hospital
Liu Haifang| Deputy Chief Physician, Department of Obstetrics and Gynecology, Huashan Hospital Affiliated to Fudan University
Wang Dong| Chief Physician of Hepatobiliary Surgery, Peking University People’s Hospital
Qu Mouwen| Chief Physician of Anorectal Department, Guang’anmen Hospital, Chinese Academy of Chinese Medical Sciences
References
[1]Haumaier F, Sterlacci W, Vieth M. Histological and molecular classification of gastrointestinal polyps. Best Pract Res Clin Gastroenterol. 2017 Aug;31(4):369-379. doi: 10.1016/j.bpg.2017.06.005. Epub 2017 Jun 27. PMID: 28842046.
[2]Tanaka S, Saitoh Y, Matsuda T, Igarashi M, Matsumoto T, Iwao Y, Suzuki Y, Nozaki R, Sugai T, Oka S, Itabashi M, Sugihara KI, Tsuruta O, Hirata I, Nishida H, Miwa H, Enomoto N, Shimosegawa T, Koike K. Evidence-based clinical practice guidelines for management of colorectal polyps. J Gastroenterol. 2021 Apr;56(4):323-335. doi: 10.1007 /s00535-021-01776-1. Epub 2021 Mar 12. PMID: 33710392; PMCID: PMC8005396.
[3]Shussman N, Wexner SD. Colorectal polyps and polyposis syndromes. Gastroenterol Rep (Oxf). 2014;2(1):1-15. doi:10.1093/gastro/got041< /p>
[4] Kim NH, Jung YS, Park JH, et al.Risk of developing metachronous advanced colorectal neoplasia after colonoscopic polypectomy in patients aged 30 to 39 and 40 to 49 years[J]. Gastrointest Endosc, 2018, 88(4): 71 5.
[5] Shanghai Anti-Cancer Association, Fudan University Affiliated Cancer Hospital. Recommendations for screening and prevention of common malignant tumors in residents [J]. Health Guidelines, 2019(6):48-49.
[6]Provenzale D, Gupta S, Ahnen DJ, et al. NCCN guidelines insights: colorectal cancer screening, version 1.2018[J]. Journal of the National Comprehensive Cancer Network, 2018, 16 (8): 939-949.
[7]Song M, Emilsson L, Roelstraete B, Ludvigsson JF. Risk of colorectal cancer in first degree relatives of patients with colorectal polyps: nationwide case-control study in Sweden. BMJ. 2021 May 4;373:n877. doi: 10.1136/bmj.n877. PMID: 33947661; PMCID: PMC8083372.
[8]Colorectal cancer screening (PDQ) ― Health professional version. National Cancer Institute. https:https://www.cancer.gov/types/colorectal/hp/colorectal-screening- pdq. Accessed Feb. 18, 2022.
[9]Chen CY, Lu CL, Chang FY, et al. Risk factors for gallbladder polyps in the Chinese population[J]. American Journal of Gastroenterology (Springer Nature), 1997, 92 (11).
[10]Xu A, Hu H. The gallbladder polypoid-lesions conundrum: moving forward with controversy by looking back[J]. Expert Rev Gastroenterol Hepatol, 2017, 11(11):1071 -1080
[11] Liu Kai, Lu Yi, Mustaba·Maimatireyimu, Dou Ningxin, Xu Mingxing, Lin Nan, Xu Ruiyun. Re-indication of surgery for gallbladder polypoid lesions Thinking-a retrospective study of 388 cases of cholecystectomy[J].Chinese Journal of Liver Surgery Electronic Journal,2021,10(02):147-152.
[12]Wiles R, Thoeni RF, Barbu ST, et al. Management and follow-up of gallbladder polyps : Joint guidelines between the European Society of Gastrointestinal and Abdominal Radiology (ESGAR), European Association for Endoscopic Surgery and other Interventional Techniques (EAES), International Society of Digestive Surgery – European Federation (EFISDS) and European Society of Gastrointestinal Endoscopy (ESGE). Eur Radiol. 2017;27(9):3856-3866. doi:10.1007 /s00330-017-4742-y
[13]Foley KG, Lahaye MJ, Thoeni RF, Soltes M, Dewhurst C, Barbu ST, Vashist YK, Rafaelsen SR, Arvanitakis M, Perinel J, Wiles R, Roberts SA. Management and follow-up of gallbladder polyps: updated joint guidelines between the ESGAR, EAES, EFISDS and ESGE. Eur Radiol. 2021 Dec 17. doi: 10.1007/s00330-021-08384-w. Epub ahead of print. PMID: 34918177.< /p>
[14]Schnatz PF, Ricci S, O’Sullivan DM. Cervical polyps in postmenopausal women: is there a difference in risk? [J]. Menopause,2009,16(3):524-528.
[15]Stamatellos I, Stamatopoulos P, Bontis J. The role of hysteroscopy in the current management of the cervical polyps [J]. Arch Gynecol Obstet, 2007,276(4):299-303.
[16]Tanos V, Berry KE, Seikkula J, Abi Raad E, Stavroulis A, Sleiman Z, Campo R, Gordts S. The management of polyps in female reproductive organs. Int J Surg . 2017 Jul;43:7-16. doi: 10.1016/j.ijsu.2017.05.012. Epub 2017 May 5. PMID: 28483662.
[17]Alkilani YG, Apodaca-Ramos I. Cervical Polyps. [Updated 2021 Sep 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan- . Available from: https:https://www.ncbi.nlm.nih.gov/books/NBK562185/
[18]McIlwaine P, McElhinney B, Karthigasu KA, et al. A prospective study of the use of the M yosure resectoscope to manage endometrial polyps in an outpatient setting[J]. Australian and New Zealand Journal of Obstetrics and Gynaecology, 2015, 55(5): 482-486.
[19]McIlwaine P, McElhinney B, Karthigasu KA, et al. A prospective study of the use of the M yosure resectoscope to manage endometrial polyps in an outpatient setting[J]. Australian and New Zealand Journal of Obstetrics and Gynaecology, 2015, 55(5): 482-486.
[20]Antunes Jr A, Costa-Paiva L, Arthuso M, et al. Endometrial polyps in pre-and postmenopausal women: factors associated with malignancy[J]. Maturitas, 2007, 57(4): 415-421.
[21]Nijkang NP, Anderson L, Markham R, Manconi F. Endometrial polyps: Pathogenesis, sequelae and treatment. SAGE Open Med. 2019 May 2;7:2050312119848247. doi: 10.1177/ 2050312119848247. PMID: 31105939; PMCID: PMC6501471.
[22] American Association of Kim NH, Jung YS, Park JH, et al. Risk of developing metachronous advanced colorectal neoplasia after colonoscopic polypectomy in patients aged 30 to 39 and 40 to 49 years[ J]. Gastrointest Endosc, 2018, 88(4): 71 5. AAGL practice report: practice guidelines for the diagnosis and management of endometrial polyps. J Minim Invasive Gynecol. 2012 Jan-Feb;19(1):3-10 . doi: 10.1016/j.jmig.2011.09.003. PMID: 22196255.
*The content of this article is for the popularization of health knowledge and cannot be used as a specific diagnosis and treatment suggestion, nor can it replace the face-to-face consultation of a licensed physician, and is for reference only.
*The copyright of this article belongs to Tencent Medical Dictionary. Unauthorized reprinting by media is prohibited. Illegal reprinting will be investigated for legal responsibility according to law. Individuals are welcome to forward to the circle of friends.