Dizziness/vertigo is a very common complaint of neurology outpatients, but there is currently a lot of confusion in the etiological diagnosis in this field, resulting in a large number of patients being misdiagnosed and mistreated.
There is a complex relationship between dizziness/vertigo and etiology (Figure 1). The main causes of dizziness/vertigo include vestibular peripheral, mental and central.
Central accounts for less than 10% of the etiology, and posterior circulation ischemia, which is part of central dizziness/vertigo, accounts for even less of all dizziness/vertigo patients, but A large number of patients with dizziness/vertigo present in the neurology department are arbitrarily diagnosed with ischemia.
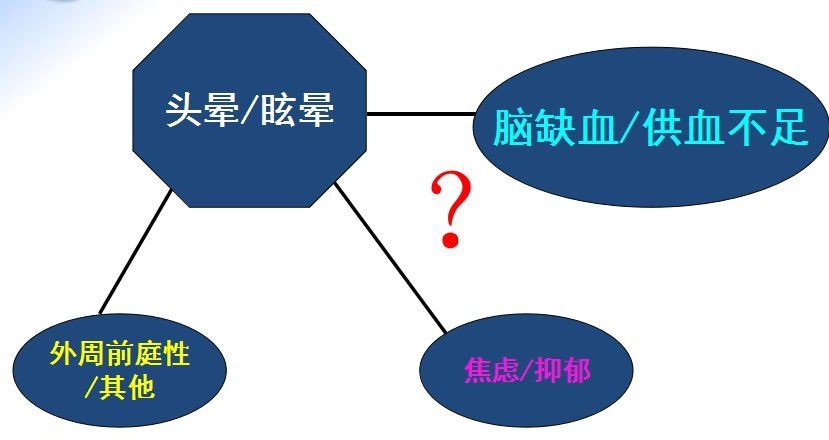
Figure 1 The complex relationship between dizziness/vertigo and etiology
If you do not want to misdiagnose and treat , as a neurologist, we must first remember these “5 tricks – 3 do not 2”:
Don’t easily diagnose patients with vertebrobasilar insufficiency (VBI);
< p> Do not easily diagnose patients with posterior circulation ischemia (PCI) or ischemic dizziness/vertigo;
Carefully evaluate the value of cerebral artery stenosis, especially vertebrobasilar stenosis in the etiological diagnosis of dizziness/vertigo;
It is necessary to recognize that transcranial Doppler (TCD) ) is not diagnostic of cerebral insufficiency.
Why is this “3 don’t 2 want”? This article takes you to analyze them one by one.
1
The concept is backward, the concept is confused
PCI only includes posterior circulation transient ischemic attack (TIA) and posterior circulation cerebral infarction, calling for no more Use VBI. There are many differences between VBI and PCI, as shown in Figure 2:
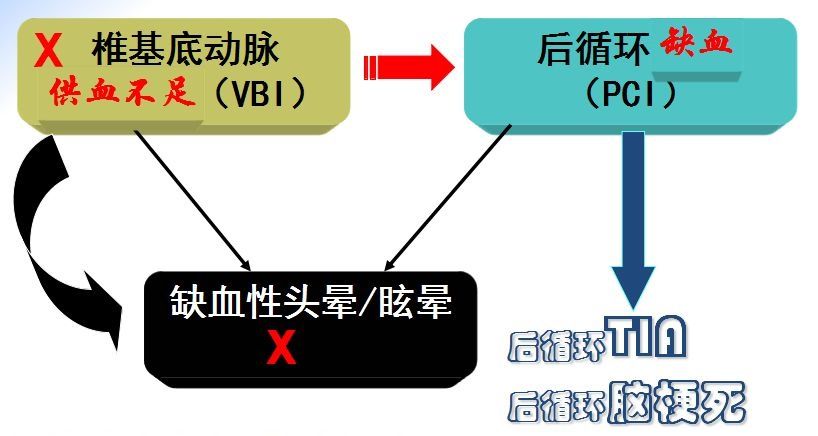
Figure 2 Differences between VBI and PCI< /p>
2
Misuse and abuse of TCD
The most misused and abused test method in neurology is TCD, and TCD is the most serious in China The error is also based on changes in blood flow velocity to make a diagnosis of “brain insufficiency”. A considerable portion of the dizziness/vertigo patients presenting to the outpatient clinic had undergone TCD.
Patients have often been suffering from dizziness/vertigo for a long time. The first sentence when they sit down is “Doctor, I am dizzy”, and the second sentence is “I have insufficient blood supply to the brain”. Then, the TCD diagnosis report will be taken out of the bag, which often reads “Vebrobasilar insufficiency”. With such a diagnosis report, the patient cannot believe that he has insufficient blood supply.
Then the question is: Can TCD diagnose cerebral insufficiency?
The answer is: No!
But the trouble is: there are many neurologists who do not know that TCD cannot diagnose cerebral insufficiency.
What’s more serious: the operator who wrote the TCD report for cerebral insufficiency does not understand that TCD cannot diagnose cerebral insufficiency. If he knew, the technician would not make such a diagnosis.
Clinicians often see the following TCD reports: ① Increased blood flow rate indicates cerebral arterial spasm; ② Slow blood flow rate indicates cerebral insufficiency.
Why is it wrong that the slowing of blood flow indicates insufficient blood supply to the brain? At least three concepts are blurred here: ① intra-arterial blood flow velocity; ② intra-arterial blood flow; ③ cerebral blood flow.

Figure 3
Blood flow velocity is not equal to blood flow through blood vessels: ① blood flow Velocity = distance of red blood cell flow per unit time (cm/s); ② blood flow through blood vessels = volume of red blood cell flow per unit time (ml/s).
Under the condition of constant blood vessel diameter, blood flow velocity is proportional to blood flow: ①fast blood flow—large blood flow; ②slow blood flow—small blood flow.
In the case of unknown vessel cross-sectional area, blood flow velocity cannot reflect blood flow.
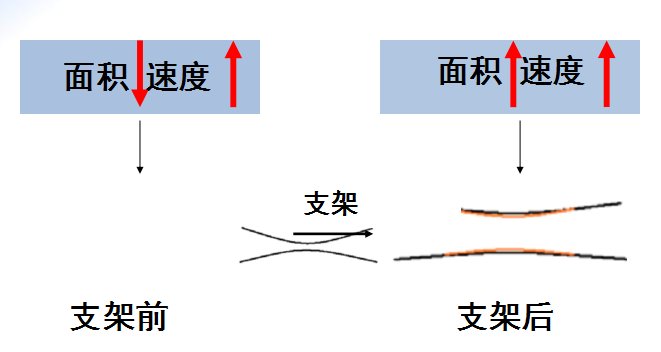
Figure 4 Before and after stent placement, the relationship between blood flow velocity and area is completely different
Could it be that the blood flow through the artery is reduced instead? In fact, it is because the blood flow through the blood vessels is not the same as the cerebral blood flow. The blood flow in an artery is not representative of the cerebral blood flow supplying that area, and a decrease in cerebral blood flow can be detected by the following tests: CT perfusion, magnetic resonance imaging (MRI perfusion, single photon emission computed tomography (SPECT), positron emission tomography Emission computed tomography (PET). Decreased blood flow in an artery does not necessarily indicate a decrease in cerebral blood flow in the area supplied by the artery (Figure 5, Figure 6).
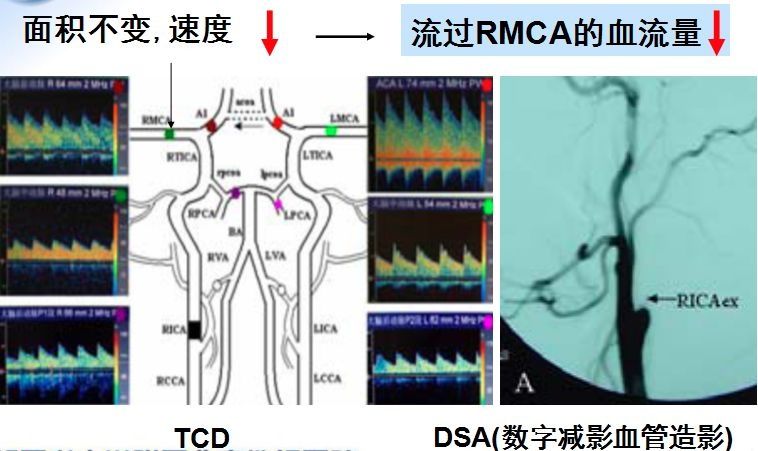
Figure 5
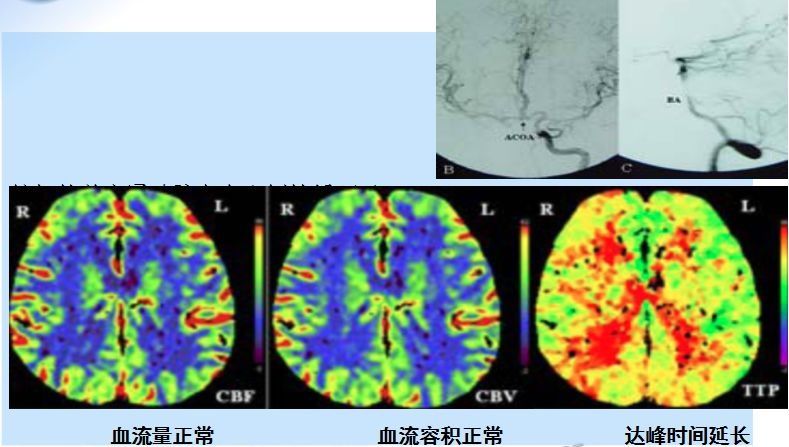
Figure 6
< p> 3
Assumption of the relationship between some abnormal test results and dizziness/vertigo
1
Cervical bone hyperplasia
Transferred from other places, to the outpatient clinicAmong the patients with dizziness/vertigo, a considerable number of them have taken cervical spine-X films, especially the elderly. The common diagnoses on cervical spine-X-ray reports include: straight cervical curvature, narrowing of the intervertebral space, and bone hyperplasia. These patients will ask themselves: “Doctor, is my cerebral insufficiency caused by cervical spondylosis?”
In fact, it is rare for cervical vertebral bone hyperplasia to oppress the vertebral artery, and it is not caused by dizziness/vertigo and posterior circulation ischemia The main reasons (shown in Figure 7). The relationship between cervical osteoarthritis and dizziness/vertigo is unclear, at least not the cause of posterior circulation ischemia.

Figure 7
2
Cavity
< p> Another phenomenon is often encountered when seeing dizzy/vertigo patients in the outpatient clinic. The first sentence of the patient when he sees the doctor is “Dr. I am dizzy”, and the second sentence may be “I have a cerebral infarction” or “I have a Cavity infarction”, and then can’t wait to take out the CT film of the head to show the doctor. The patient’s meaning is very clear: my dizziness/vertigo is caused by the caval infarction in the brain, doctor, please see how to treat my dizziness/vertigo by treating my caval infarction.
An elderly person with several small infarcts or ischemia on head CT or MRI if he has one or more of the risk factors such as hypertension, hyperlipidemia, diabetes or smoking The stove is not surprising.
The clinical manifestations of cavitary infarction are as follows, none of which says simple dizziness or vertigo!
pure motor stroke;
pure sensory stroke;
ataxia hemiparesis;
sensorimotor stroke;
Articulation Clumsy Hand Syndrome.
3
Cerebral artery stenosis
Now more and more doctors know the importance of vascular imaging examination, and many patients have vascular imaging, so there are Could cerebral artery stenosis explain the patient’s dizziness/vertigo? It is easy to fall into another misunderstanding here, relying too much on auxiliary examinations and ignoring consultations!
Summary full text: After reading it, do you understand why it is “3 don’t 2 want”? One last repetition:
Don’t make a patient diagnosis of VBI again
Don’t make a second diagnosis of PCI or ischemic dizziness/vertigo
Don’t make a mistake Cervical vertebral bone hyperplasia and lacunar cerebral infarction are closely related to dizziness/vertigo
The value of cerebral artery stenosis, especially vertebral and basilar artery stenosis in the etiological diagnosis of dizziness/vertigo should be carefully evaluated< /p>
It should be recognized that TCD cannot diagnose cerebral insufficiency
This article is compiled from the lecture “Differential Diagnosis of Dizziness and Cerebral Insufficiency” by Professor Du Zhigang of Beijing Ditan Hospital Affiliated to Capital Medical University. Medical Doctor Station”, search the title to watch the full lecture video.
This article was first published: Medical Neurology Channel