Venous thromboembolism (VTE) is a common complication in hospitalized patients. At present, compared with internal medicine, Chinese surgery has a stronger awareness of prevention, and the onset of VTE in internal medicine patients is usually hidden, and the clinical symptoms are not obvious. Therefore, scientific and standardized evaluation of VTE in medical patients is particularly important.
1 Definition
VTE mainly includes deep vein thrombosis (DVT) and pulmonary thromboembolism (PTE).
The former usually occurs in the deep veins of the lower extremities, and may be asymptomatic or local pain and distal edema may occur. Proximal DVT above the N vein is an important source of PTE emboli.
The latter is mainly caused by a thrombus from the venous system or the right heart blocking the pulmonary artery or its branches. It can cause breathing difficulties, circulatory disorders, chest tightness, chest pain, etc., and even life-threatening.
2 Risk Factors
The mechanism of VTE is blood stasis, vascular endothelial injury and hypercoagulability, namely the three elements of Virchow. Almost everyone in hospitalized medical patients has a high-risk factor.
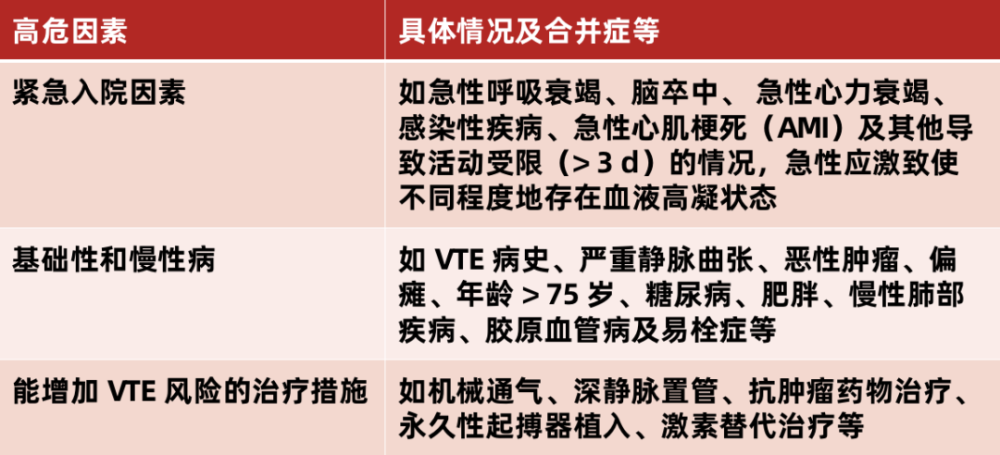
Note: Patients with two or more risk factors are at higher risk for VTE.
3 Risk Assessment
Current domestic and international guidelines recommend VTE risk assessment for all medical inpatients, and the need for VTE prevention should be considered based on the assessment results.
Currently, the standards for VTE risk assessment of inpatients in internal medicine are not exactly the same. Among them, the Padua risk assessment model is recommended by most guidelines, and now “Chinese Expert Recommendations on the Prevention of Venous Thromboembolism in Inpatients in Internal Medicine” This model is also used, as follows:

Padua Model Score
But there are some situations that are not applicable to Chinese people, mainly:
One risk factor in this model is factor V Leiden mutation and prothrombin G20210A mutation, which occur in 1% to 6% of the Caucasian population, but are very rare in the Chinese population ;
The model has a total of 11 risk factors, of which 4 items, including advanced age, AMI/ischemic stroke, obesity, and use of hormone therapy, have no significant difference between high-risk VTE patients and non-VTE patients. Effectively distinguish potential VTE and non-VTE patients, so it is difficult to accurately predict the occurrence of VTE.
4 The value of biomarkers
1) D-dimer
D-dimer acts as a marker of activation of the coagulation and fibrinolysis system, which can indirectly reflect thrombotic activity. Has a high negative predictive value in acute VTE. Used in combination with the Wells score in clinical practice, it can help rule out or confirm VTE.

▲ Wells Score Scale
Wells total score < 2 and D-dimer negative can rule out the diagnosis of DVT; when the total score is ≥ 2 and D-dimer is positive, the diagnosis of DVT is considered.
D-dimer levels in the body increase with age. The current D-dimer thresholds are as follows:
The degree of increased D-dimer also indicates the degree of coagulation state, and the value of Wells score can also be used as a predictor of future recurrent VTE. At the same time, the higher the Wells value, the higher the risk of VTE recurrence.
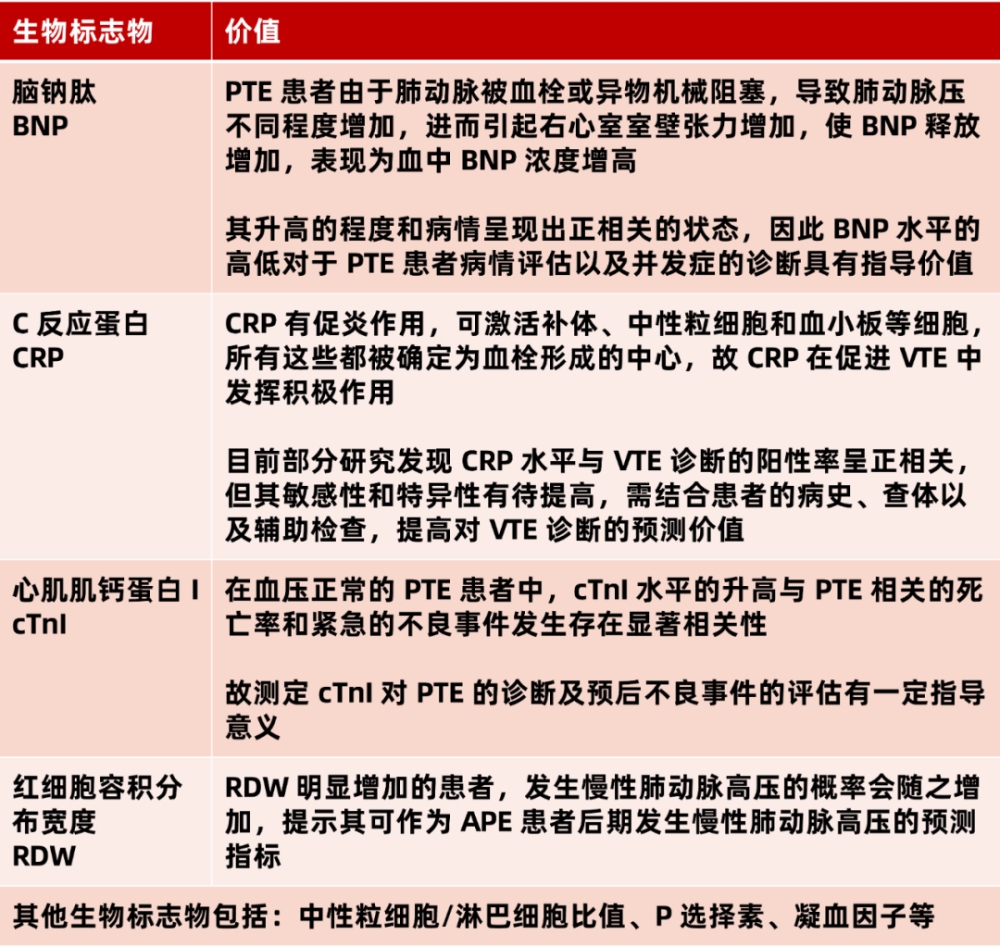
2) Other important biomarkers
5 Active Prevention
Before VTE prevention, it is necessary to conduct a comprehensive assessment of the patient, control the patient’s underlying disease, and clarify the patient’s concomitant medication. For patients who use anticoagulant drugs, antiplatelet drugs, thrombolytic drugs, etc. at the same time, which may increase the risk of bleeding, the dose should be reduced as appropriate, or bridge therapy should be started as soon as possible.
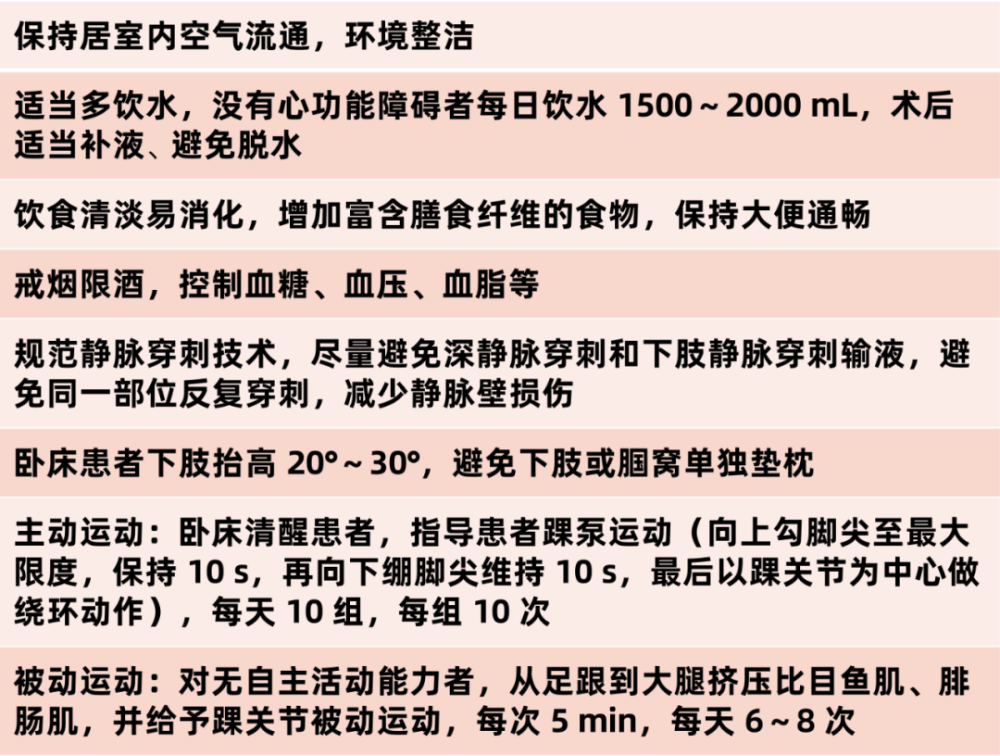
1) Basic Prevention
Basic Prevention
Because of the particularity of inpatients in internal medicine, active basic prevention can play a certain positive role.
Mechanical prevention
Mechanical prevention includes graded compression stockings, intermittent pneumatic compression devices, and plantar venous pumps. For those with contraindications to mechanical prophylaxis, mechanical prophylaxis alone cannot replace drug prophylaxis.
Contraindications to mechanical prophylaxis: severe lower extremity arteriosclerosis, congestive heart failure, pulmonary edema, lower extremity DVT (except GCS), thrombophlebitis, severe local lower extremity lesions such as dermatitis, gangrene, severe deformities, etc.
Patients without contraindications to mechanical prophylaxis are advised to prevent VTE by:
Without contraindications to the use of anticoagulants, it is recommended to combine mechanical prophylaxis with drug prophylaxis;
Mechanical prophylaxis alone is recommended for bleeding disorders or bleeding risk;
Prophylaxis on the contralateral limb can be performed if mechanical prophylaxis is not feasible or appropriate for the affected limb.
2) Drug prevention
In hospitalized medical patients with risk factors, the risk of thrombosis and bleeding must be carefully weighed:
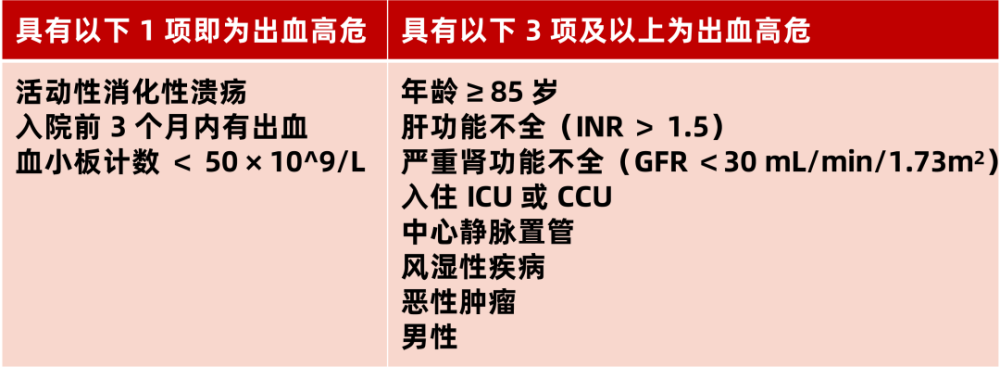
If there is no contraindication, according to the patient’s condition, one of the following drugs can be selected for prevention:
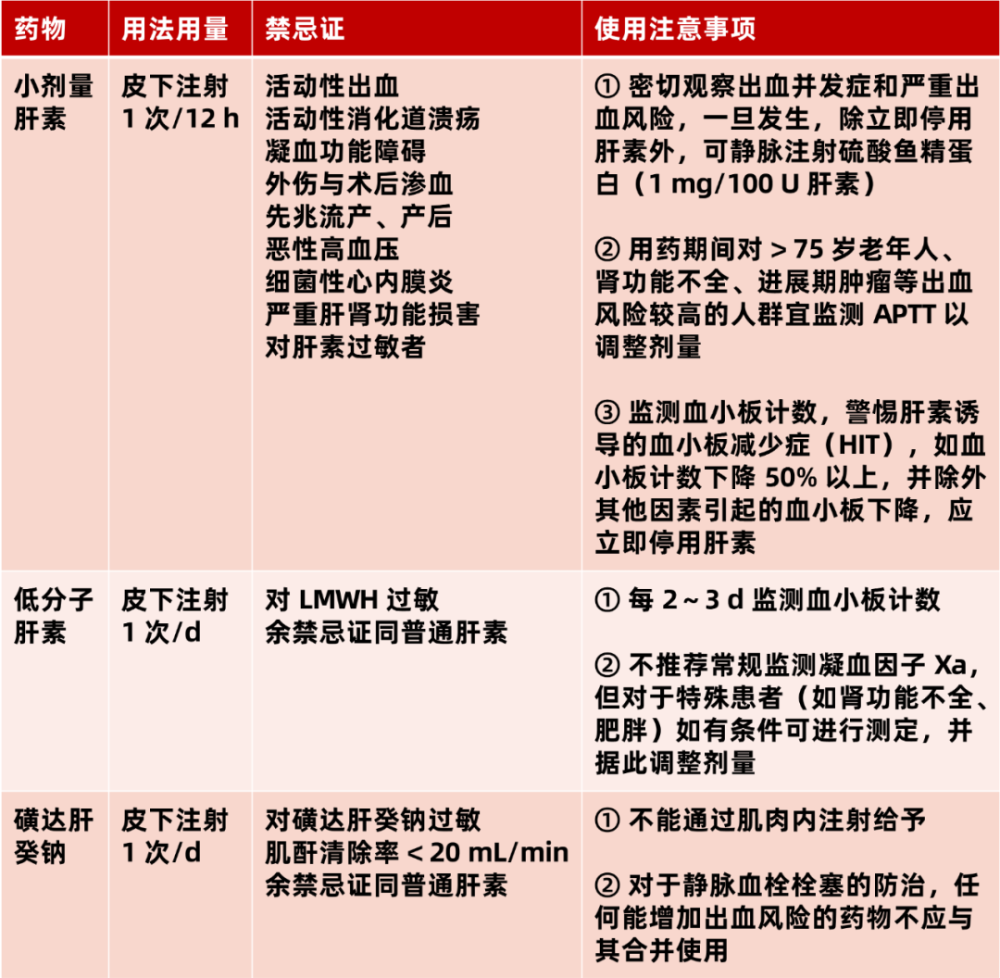
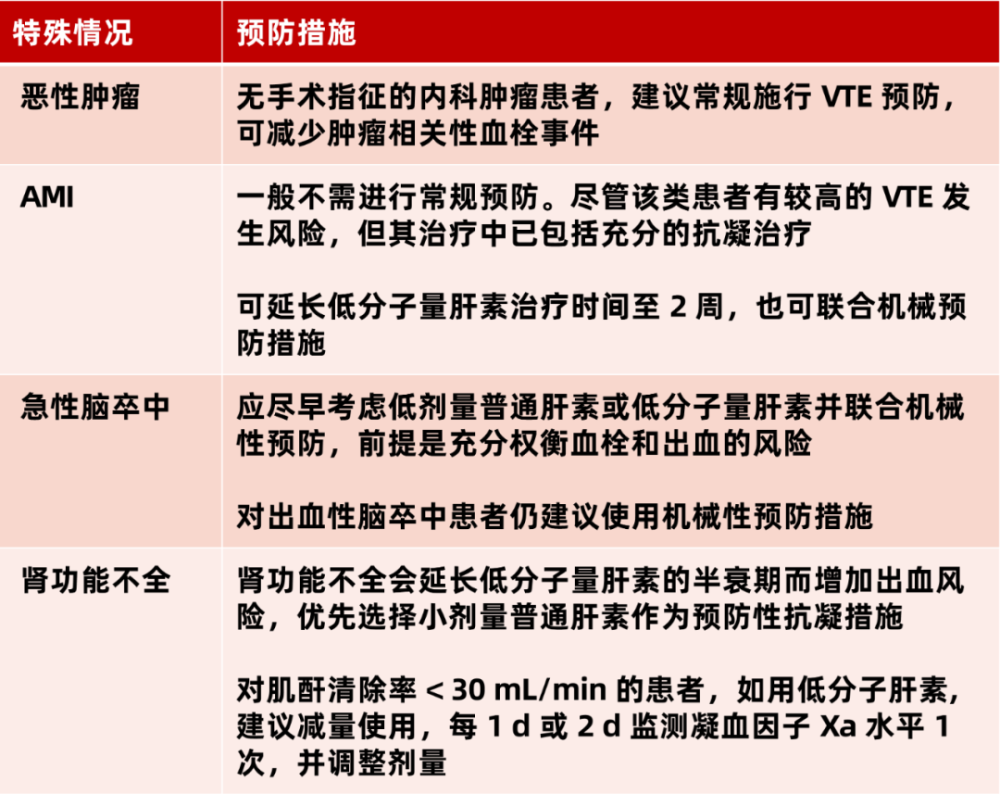
Some patients requiring special precautions:
References:
1. Zhang Peng, Liu Jinbo, Wang Hongyu, Research progress of the application value of different biomarkers in venous thromboembolism, Advances in Cardiovascular Diseases, Vol. 42, No. 11, Nov. 2021 period.
2. Ma Ping. Research progress of VTE risk assessment and prevention in medical inpatients [J]. General Nursing, 2021,19(32):4496-4499.
3. Geriatrics Branch of Chinese Medical Association, Chinese expert advice on the prevention of venous thromboembolism in internal medicine inpatients (2015), Chinese Journal of Gerontology, 2015, 34(4): 345-352 .
4. China Health Promotion Fund, Recommendations on Prevention and Management of Venous Thromboembolism in Hospitals (2018), Chinese Journal of Medicine, 2018, 98(18): 1383-1388.
Planning: ly
The source of the title map: Zhanku Hailuo
This article was first published on the professional platform of Lilac Garden: Cardiovascular Time