*For medical professionals only
Young mother died after 4 years of battle with cancer. Is this cancer really so intractable?
Writing | Strongly
Source | “Medical Oncology Channel” Public Account
The young and beautiful Sarah was diagnosed with intrahepatic bile duct cancer when her son was only 18 months old.
Because of the lack of routine screening methods for cholangiocarcinoma and the non-specific clinical features, only 25% to 30% of patients can be diagnosed at an early stage of the disease and the tumor is resectable, when there is no standard treatment plan. At this time, Sarah seemed to be trapped on the edge of a cliff, and there was an abyss with no end in sight.
Sarah’s 4-year battle with cancer was published in the top medical journal, The New England Journal of Medicine. Surprisingly, Sarah’s parental testimonials are rarely published at the end of the case report.
Unexplained acute abdominal and back pain hits the door
Sarah used to be in good health, but 3 years ago she had sudden abdominal pain and back pain, so she went to a hospital for a checkup. Imaging studies suggest primary or metastatic carcinoma, and pathological biopsy shows moderately differentiated adenocarcinoma, and these features are consistent with the diagnosis of intrahepatic cholangiocarcinoma in the absence of an extrahepatic primary tumor.
But Sarah simply didn’t have time to accept the bolt from the blue, and more difficult questions awaited her.
Most liver tumors spread from a primary site outside the liver, and only a few tumors develop inside the liver. The most important thing at the moment is to distinguish between metastatic adenocarcinoma and cholangiocarcinoma, Sarah’s classic immunohistochemical patterns CK7+, CK19+ and CK20 can also be found in patients with pancreatic, gastric, small bowel and, less commonly, colon metastases.
However, hematoxylin-eosin staining of tumor specimens provided critical evidence for the diagnosis of Sarah’s cholangiocarcinoma (Figures 1A and 1B), a cholangiocellular pattern that is a distinguishing feature of cholangiocarcinoma.
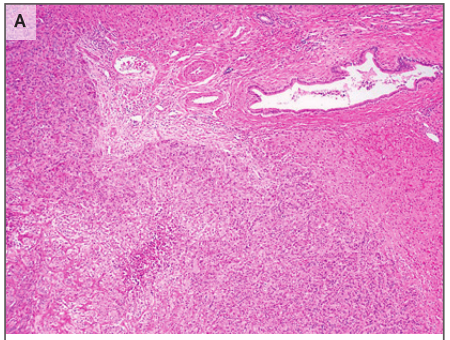
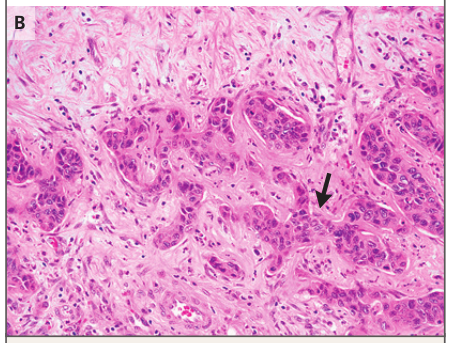
Figure 1: Tumor Specimen
Figure 1A (upper right panel): Hematoxylin-eosin staining showed poorly differentiated adenocarcinoma and adjacent liver tissue;
Figure 1B (arrow): Under high magnification, tumor cells are arranged in a bile duct pattern similar to antlers
Later, Sarah underwent extended right hepatectomy and Roux-en-Y hepatojejunostomy with the aim of curing the disease. Pathological examination showed adenocarcinoma of 6.5 cm × 6.5 cm × 6.0 cm with 3 satellite nodules ranging in diameter from 0.3 to 1.4 cm. The margins were negative, but close to the tumor (distance between margin and tumor <1 mm), and 3 lymph nodes were negative.
Postoperative adjuvant therapy may have saved her life
Bile duct cancer is rare in the United States, with only about 8,000 cases per year. Sarah’s sudden abdominal pain is one of the most common manifestations of cholangiocarcinoma, which can also manifest as weight loss, nausea, loss of appetite or occasional jaundice.
The recurrence rate of cholangiocarcinoma after resection is as high as 60%. In order to improve the cure rate, Sarah can only consider adjuvant chemotherapy to remove micrometastases. Data from the BILCAP trial support the use of capecitabine as adjuvant therapy for patients after cholangiocarcinoma resection; in the per-protocol analysis, the overall survival rate of patients in the capecitabine group was significantly higher than that in the active surveillance group.
Sarah started adjuvant gemcitabine and cisplatin 2 months after surgery, before the results of the BILCAP trial were available.
Cancer is not a nightmare for her, but a push to love life
12 months after the end of adjuvant therapy, CT surveillance revealed a new lesion (1.4 cm in diameter) in the left hepatic lobe with features consistent with recurrence of cholangiocarcinoma (Figure 2A). Sarah was enrolled in a phase I clinical trial of an OX40 agonist, but discontinued treatment after 3 months due to liver disease progression (Figure 2B). At this time, biopsy of the liver lesion confirmed recurrent metastatic cholangiocarcinoma.
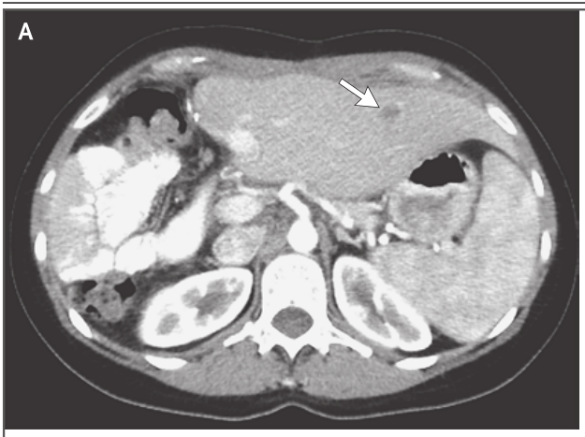
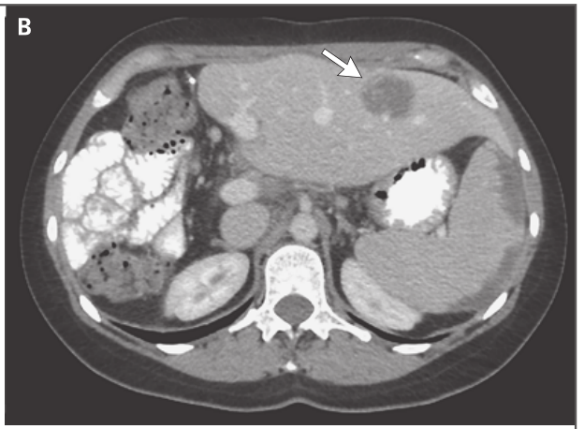
Figure 2: CT image of liver after adjuvant therapy
Figure 2A (arrow): a new low-density lesion with a diameter of 1.4 cm in the left hepatic lobe;
Figure 2B (arrow): Tumor enlargement, consistent with disease progression
Another sap, has the road to adjuvant therapy and clinical trials come to an end?
Sarah was restarted on gemcitabine and cisplatin before developing an allergic reaction to cisplatin. To clarify the staging again, imaging studies showed progression of the liver lesion, the previously observed liver lesion was now 3.6 cm in diameter, and a second liver lesion of 1.5 cm in diameter appeared. New pulmonary lesions of undetermined significance, <1 cm in diameter, were also identified. The doctor performed microwave ablation on the liver lesions. The interval between the two microwave ablations was 1 month. Postoperative enhanced CT showed no enhancement in the ablation zone (Figure 3C). Fortunately, this treatment was effective.
Sarah’s two well-defined cancer lesions have been treated effectively, but she can’t sit back and relax, and she’s going to start active surveillance. Although the treatment in the past period has encountered bumps, it still maintains the trend of making progress while maintaining stability. However, the next thing has changed drastically.
PET-CT 3 months later revealed two new lesions with FDG uptake in the left hepatic lobe, and no other FDG uptake sites. So Sarah underwent a left partial hepatectomy, and pathological examination confirmed the recurrence of cholangiocarcinoma.
5 months after surgery, CT of the chest, abdomen, and pelvis showed multiple new lesions in the liver (Fig. 3D), up to 3.0 cm in diameter, and multiple new lesions in the lungs and enlarged lesions, with a maximum diameter of 1.2 cm. Cholangiocarcinoma has recurred…
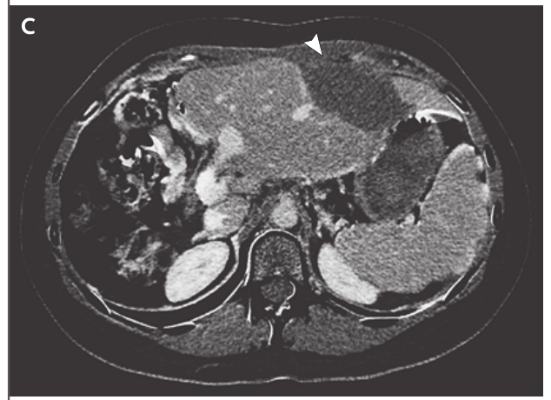
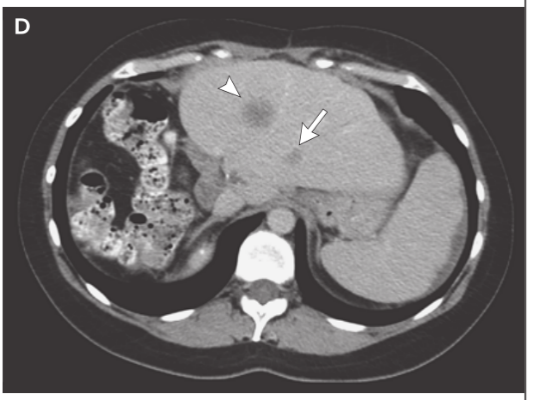
Figure 3: Liver CT Image
Figure 3C (arrow): After two microwave ablation, there is no enhancement in the ablation area;
Figure 3D (arrow): Multiple new hypodense liver lesions
At this point, there seems to be no turning point, and Sarah has not fallen. She went to the Massachusetts General Hospital outpatient clinic for evaluation and treatment. Sarah, who suffered from cancer at a young age, is lonely and struggling with treatment, but her willingness to show her vulnerable side has won her a lot of social support. Sarah’s parents testify in the New England Journal of Medicine that their daughter actively sought out connections and created the “cholangiocarcinoma warriors” group, which gave her a sense of belonging and is still used by hundreds of others Patients bring a sense of belonging.
Immunotherapy and targeted therapy were not friendly to her
The combination of gemcitabine and cisplatin has been the standard first-line treatment for patients with recurrent or unresectable cholangiocarcinoma for over a decade. But Sarah had progressed after receiving this regimen when her bile duct cancer recurred, so she had to turn her attention to two other classes of drugs used to treat solid tumors: immunotherapy and molecularly targeted drugs.
In contrast to traditional chemotherapy, immunotherapy can lead to long-term remission and even occasionally cure patients. In 2017, the U.S. Food and Drug Administration (FDA) approved pembrolizumab for unresectable or metastatic refractory disease with mismatch repair deficiency or high microsatellite instability solid tumor patients. Sarah has a tumor with mismatch repair function, stable microsatellites, and rapid progression during immunotherapy. Immunotherapy does not seem to work.
Targeted drugs rely on the detection and inhibition of specific molecular changes that are critical for tumor survival. In 2020, pemigatinib, an oral fibroblast growth factor receptor (FGFR) small-molecule inhibitor, became the first FDA-approved drug specifically for the treatment of cholangiocarcinoma.
Doctors analyzed the tumor’s molecular expression profile and found that Sarah’s chromosome 10, FGFR2, and chromosome 12, POC1B, had an in-frame fusion between chromosomes. Activation of the FGFR pathway drives a series of intracellular events leading to tumorigenesis, proliferation, and cell migration. In addition, pemigatinib has not been approved by the FDA during Sarah’s treatment, and there is no standard treatment for cholangiocarcinoma. Targeted therapy is no longer the case.
She finds a way through the thorns
This time, behind bars, Sarah sees new hope. A Phase I, first-in-human clinical trial of the covalently conjugated oral FGFR inhibitor futibatinib is enrolling patients. The doctors discussed in detail the concept of molecularly targeted therapy, as well as the risks and benefits of this therapy. Sarah’s parents also said they knew from the start that the benefit of the trial drug had not been proven, but Sarahh thought and signed the informed consent form to participate in the trial.
Sarah has the greatest drive and enthusiasm despite all the unknowns that await her. “Our daughter wants to live as long as possible through the trial. She wants to spend more time with her son. She is a true mother. She feels that participating in research will improve the treatment of not only herself, but also other patients. She trusts the judgment of her physicians, and she trusts that if she feels unwell during the trial, the team of clinicians will take good care of her,” Sarah’s parents said in a testimonial to the New England Journal of Medicine.
She experienced side effects such as mild diarrhea and nausea during treatment, but fortunately there were few other complications. After 6 weeks of futibatinib treatment, follow-up CT showed that multiple lesions shrank or disappeared (Figure 4E). According to RECIST v1.1, Sarah’s tumor burden decreased by 37% overall, and the tumor burden was controlled for 7.2 months. CT showed mixed responses, with multiple new or growing lesions in the liver and lung (Fig. 4F), while others regressed.
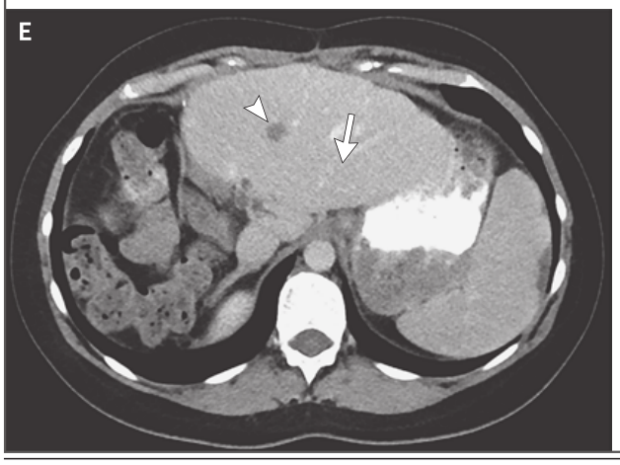
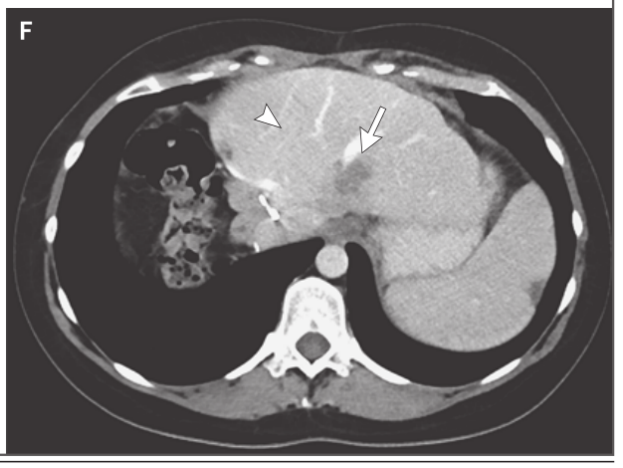
Figure 4: Liver CT Image
Figure 4E (arrow): one lesion was significantly reduced in size and the other metastases were significantly reduced in resolution; Figure 4F (arrow): multiple new or growing livers appeared Lesion
After disease progression, Sarah participated in a phase I clinical trial of TNO155, a SHP2 (Src homology 2 domain-containing protein tyrosine phosphatase 2) inhibitor. After she developed fever and malaise and was diagnosed with pneumonia, TNO155 was discontinued. While receiving treatment for pneumonia, her symptoms persisted for a month. CT at that time showed enlarged liver and lung metastases and new lymphadenopathy in the upper abdomen.
With no other treatment options available, Sarah received hospice care 4 years after her initial diagnosis of bile duct cancer. Two months later, she passed away peacefully accompanied by her family.
The long drive from New Jersey to Boston to participate in a clinical trial brings Sarah’s four difficult years to an end. As Sarah’s parents said, “Although cancer makes most patients feel like they are standing on the edge of a cliff, there is no shortage of powerful forces in clinical practice and scientific research to find a cure, and everyone has reason to hope.”
References:
[1]. Goyal Lipika,Chen Christopher T,Pierce Theodore T et al. Case 8-2021: A 34-Year-Old Woman with Cholangiocarcinoma.[J] .N Engl J Med , 2021, 384: 1054-1064.
Source: Medical Oncology Channel
Editor in charge: Zheng Huaju
Proofreading: Zang Hengjia
Plate making: Xue Jiao