The author of this article: Tun Tun
Writing medical records is a compulsory course for every doctor entering the clinic.
On a sunny afternoon, the young doctor Gu Pei sat in front of the computer and made up the medical records. For a whole year, no one recorded the daily course of this patient.
On another sunny afternoon, the younger interns took the director’s signature and signed the medical record blankly in the reviewer column. As for this “” The professionalism of “Memoirs” has long exceeded the ability of an intern.
I opened the medical record and checked it. There was no signature on the medical record. The word “quality control” was written on each page crookedly. I couldn’t sleep horizontally and vertically. It can be seen from the cracks that “loopholes” are written all over the book.
Copy-Paste Medical History
Major medical records, first trips, attending ward rounds, chief ward rounds… The producers behind these medical records are often regular doctors. Xia Yiyi (pseudonym), a training student at a tertiary hospital in Shanghai, mocked herself and said, “Our little doctor is a full-time doctor who writes medical records.”
Repetitive medical record writing has turned the regular trainees into mechanized production workers. When the surgical department rotates, Xia Yiyi will directly use the account of the superior doctor to write the course of the disease. “If there are no complications or special circumstances in minor operations, most of the medical records are similar, so we will just copy the template.”
But there are also differences from department to department. Qiu Sisi (pseudonym), who trained in a tertiary hospital in Zhejiang Province, said that during the rotation of the ICU, the higher-level doctors will not give account permissions to the lower doctors at all.
A survey of pediatric medicine residents in the United States found that 89% of physicians use the copy-and-paste feature when writing their medical records. Another study of ICUs showed that 82% of the medical records written by residents and 74% of the medical records written by the attending physicians, more than 20% of the content of the analysis and evaluation of the disease was copied and pasted, and most medical staff admitted The content imported in the medical records is inconsistent and inaccurate.
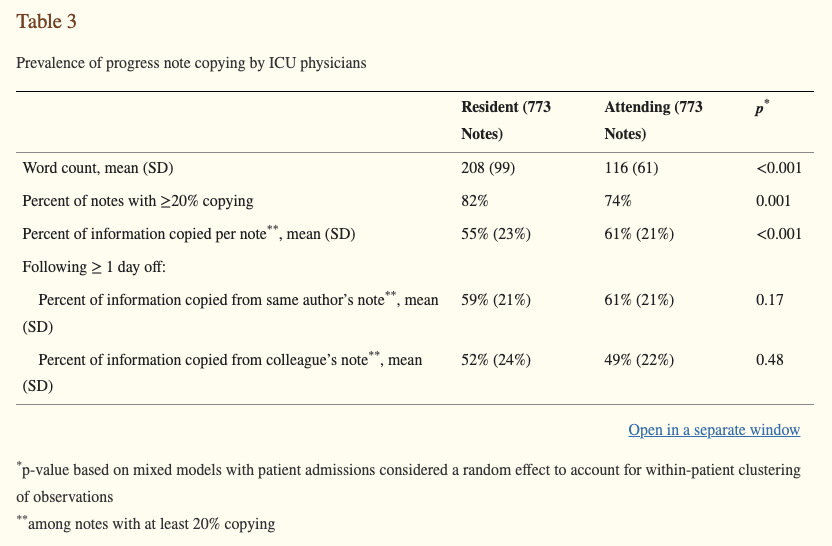
Prevalence of ICU physician copying of course records
Image source: Reference [1]
Copying against the template may also be a helpless measure when the workload is almost saturated.
A survey on the workload of Chinese doctors entering medical records shows that 46.23% of doctors need to write medical records for more than 3 hours a day, and 27.99% of doctors spend 2 to 3 hours writing medical records. between hours.
There is a natural tension between a well-developed medical record and the limited energy of the clinician. Xia Yiyi said that only in the case of complicated operations, the chief surgeon will make his own records.
In order to reduce the burden of writing medical records for doctors, “medical record scribes” were created in the United States. Trained in medical information management, these scribes assist physicians in recording medical records in real time, and sometimes in collecting test results and communicating with referring physicians.
One study showed that doctors worked 5.1 hours less per week when they were staffed with scribes. Another study of emergency departments noted that the presence of scribes significantly reduced the time physicians spent filling out rotation records.
Department quality is unguarded
Gu Pearson, who writes a large number of medical records, is still in the “training” stage in theory, and all behaviors and signatures need to be taught by teachers. But in fact, there are not many superior doctors who really control the quality of medical records written by Gu Peisheng.
When Qiu Sisi’s classmates rotate in the orthopaedic department, the director of the spine group will check the medical records of each patient, “But this is very rare, and I myself have almost never been in contact with people who deliberately check the quality of medical records. “
Tong Qiqi (pseudonym), a training student in a tertiary hospital in East China, recalled that during a month of rotation in a certain department of orthopedics, because it was a simple template copy, almost no one had seen his writing course of disease.
According to the three-level medical record quality control system of most hospitals, the first-level quality control is composed of the department director and the head nurse, who are responsible for the connotation quality and writing standard inspection of medical records in the department.
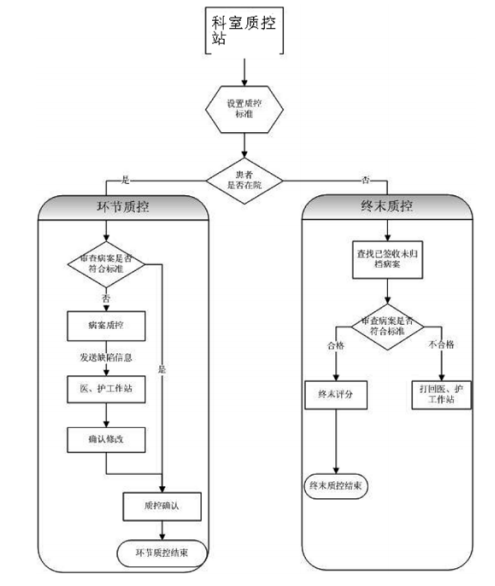
Quality control process of medical records in a tertiary hospital
Image source: Reference [5]
Data from the National Health and Health Statistical Yearbook shows that in 2018, the number of hospital admissions in tertiary hospitals was 92 million, the average hospital stay was 9.6 days, and the occupancy rate of hospital beds was 97.5%.
Behind the huge number of inpatients, the corresponding medical record review is also a huge workload. Xia Yiyi said, “Because the medical records are written with the account of the superior doctor, the superior doctor’s signature is also required when sorting them out.Words, But the volume of medical records is too large, in most cases we sign off while sorting out. ”
Gu Pearson’s mobility also brings new problems to medical record management. When the accumulated medical records are found to need to be revised when they are sorted out, Gu Pearson who filled in the medical records at that time may have already been rotated to other departments, and the doctor who can be responsible for the wrong medical records cannot be found.
Even if the medical records are written by the attending doctor or above, the review work of leaving the department is sometimes about nothing. Many interns have had the experience of holding the signature and seal of the superior doctor and burying it in the thick medical record, and covering it all afternoon.
But the risk rises sharply.
The quality control of medical records not only serves the doctor’s diagnosis and treatment behavior, but also protects the doctor. As one of the important legal documents, medical records play a pivotal role in medical disputes.
Medical damage liability follows the Principle of Fault Liability. If medical records are written irregularly or even forged or tampered with, and the medical record materials are incomplete, the medical records are found to be untrue and illegal in the medical damage lawsuit. The court can presume that the medical institution is at fault, and the hospital will lose the lawsuit and assume the responsibility for medical damage compensation. .
In the 2021 National Big Data Report on Medical Injury Liability Dispute Cases released by the Medical Law Center, medical record issues are the third largest reason for doctors to lose cases, accounting for 10%.
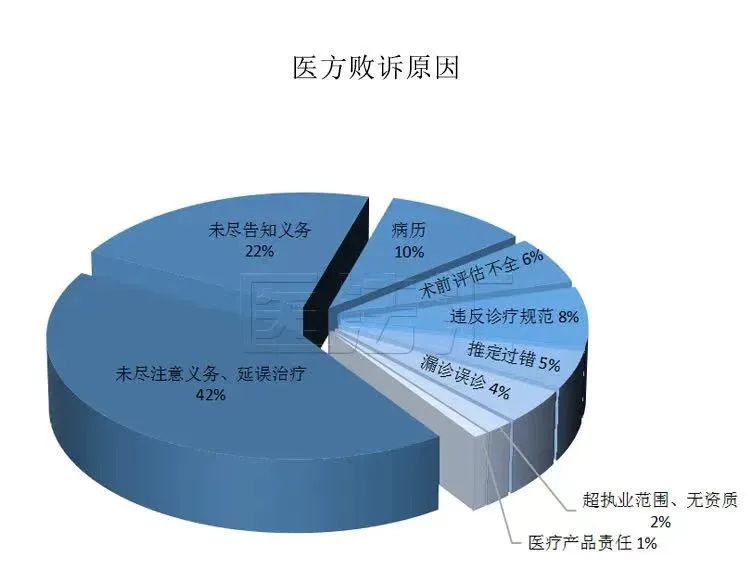
Image source: Medical Law Institute
Among them, 33% of the cases were affected by the medical party’s responsibility ratio due to the non-standard writing of medical records. Correspondingly, only 20% of the cases determined by the court to be flawed in the writing of medical records did not affect the determination of the responsibility of the medical institution.

Image source: Medical Law Institute
As a result, although many hospitals are relatively loose in the review of routine medical records, when death is involved, they will strictly check the connotation and quality of relevant medical records and document specifications.
Xia Yiyi said, “If we encounter patients who show distrust of doctors, we will also be very careful about the medical records of these patients.”
Signature of medical records is worth every word
The various medical records, after passing through the doctors and nurses in the department, finally flowed to the medical record room. As the medical record department of the bottom-line department, it usually only checks missing pages and few words, and does not check the quality of medical records.
Some doctors even said that the medical record room of their hospital is like a file room, which only stores medical records and does not conduct examinations at all.
The doctor in the medical record room also has his own helplessness. In the message of Dingxiangyuan Weibo, a doctor said that he found that the medical record was missing and returned it to the doctor, but the other party disagreed and said, “Wait for the patient to make a copy. Find me to sign again.”
But it is precisely these few signatures that no one cares about that will cause a lot of trouble for doctors.
Last year, the Tangshan Municipal Health Commission imposed administrative fines of 35,000 yuan and 50,000 yuan on the two hospitals respectively due to irregular medical records.
Dr. Song, director of neurosurgery at a tertiary hospital in Henan in 2020, did not sign the informed consent form for surgery, nor did he sign the surgical records within 24 hours after surgery. Four months after the patient was discharged from the hospital, he found that his signature was missing when copying his medical records, and complained to the Zhengzhou Municipal Health Commission.
According to the requirements of documents such as “Quality Specification for Data Filling on the Homepage of Inpatient Medical Records”, “Quality Control Indicators for Medical Record Management”, and “Basic Specifications for Writing Medical Records”, Zhengzhou Municipal Health Commission believes that Dr. Song’s behavior is inappropriate In compliance with the regulations, Dr. Song was fined 15,000 yuan.
Dr. Song believes that the diagnosis and treatment behavior itself did not cause harm to the patient, and 15,000 yuan is an excessive punishment for one less signature. After the prosecution and appeal, the court of second instance recently issued a verdict, upholding the administrative penalty imposed by the Zhengzhou Municipal Health and Health Commission, arguing that “If the punishment scale is relaxed for the behavior of not filling out the medical records according to the regulations, it is not conducive to the establishment of doctors who strictly follow the professional norms. Practice ethos can easily lead to medical disputes.”
The medical record carries all the medical information of the patient, covers the change of the patient’s condition, and is closely related to the medical safety of the patient. It is the basis for the entire diagnosis and treatment activities of medical staff, and is also the source of clinical research data.
In 2000, the American Council for Medical Research on Quality in Healthcare published a document stating that as many as 98,000 Americans die each year from preventable medical errors, including adverse drug reactions, improper blood transfusions, wrong surgery, Wrong patients, falls, pressure ulcers, etc., the reason is the lack of integration of the US medical system and the lack of interoperability of medical record information.
The layers of quality control we have established for medical records, but when we look closely, there are layers of loopholes. From training doctors copying and pasting medical records to formal review checkpoints, there are both patients and doctors who take risks.
Thanks:This article has been professionally reviewed by lawyer Mao Yunfeng of Beijing Jingshi (Shanghai) Law Firm
Planning: yuu. |Producer: gyouza
The source of the title map: I took it by myself
References:
[1] Thornton J D, Shold J D, Venkateshaiah L, et al. Prevalence of copied information by attendings and residents in critical care progress notes[J]. Crit Care Med, 2013,41( 2):382-388.
[2] Fei Fei, Qu Lili, Zhao Hai. Change?! 46% of physicians write medical records nearly 40% of their time at work Released[J]. Chinese Medical Science, 2017,7(21):1-8.
[3] Earls ST, Savageau JA, Begley S, Saver BG, Sullivan K, Chuman A. Can scribes boost FPs’ efficiency and job satisfaction? J Fam Pract. 2017 Apr;66( 4):206-214.
[4] Hess JJ, Wallenstein J, Ackerman JD, Akhter M, Ander D, Keadey MT, Capes JP. Scribe Impacts on Provider Experience, Operations, and Teaching in an Academic Emergency Medicine Practice . West J Emerg Med. 2015 Sep;16(5):602-10.
[5] Zhang Yudong. Construction and effect evaluation of three-level medical record quality control management system [J]. China Health Industry, 2017,14(26):48-50.
[6] America I O M U. To Err is Human: Building a Safer Health System[M]. Washington (DC): National Academies Press (US), 2000.
[7] Zhang Chongfei. Research on the influencing factors of medical record quality and its relationship with medical quality [D]. Air Force Military Medical University, 2019.
[8] Judgment document: (2022) Yu 01 Xingzhong No. 315