*For medical professionals only
A detailed case study is attached.
A young person suddenly suffers from myocardial infarction. Familial hypercholesterolemia is usually the first thing that comes to mind. In this case, there is no related genetic disease in the family. Unfortunately, the patient suddenly developed chest tightness. , chest pain and other symptoms, diagnosed with myocardial infarction, what is the reason? Let’s take a look.
Summary of medical records
A 27-year-old thin male patient came to the emergency department urgently for 5 hours due to chest tightness, chest pain, and shortness of breath, and asked for a detailed medical history. The patient had chest tightness after intermittent activity half a year ago, no chest pain, rest It can be relieved later, but it is not paid attention to.
5 hours ago, the patient had sudden chest pain without obvious incentive, which was crushing pain with shortness of breath, no radiating pain in the shoulder and back, and no obvious abnormality in the physical examination. The emergency doctor first thought of acute heart attack.
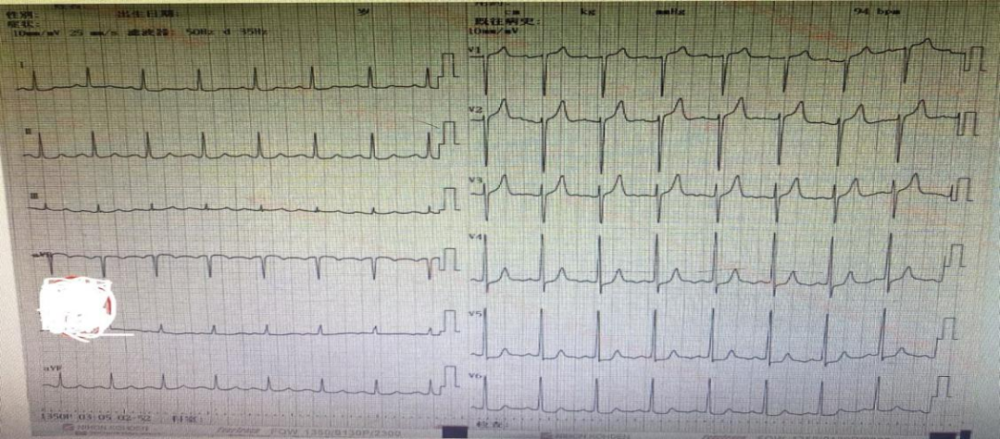
Urgent investigation of troponin T positive, electrocardiogram: sinus rhythm, V4-V6 ST depression, consider acute non-ST elevation myocardial infarction of coronary heart disease, give double anti-coagulation and other treatment , with the consent of the family, contact the catheterization laboratory, emergency interventional treatment.
Continue to inquire about the medical history in detail. The patient occasionally smokes, has no history of taking other drugs, has no related family genetic history, and has no familial hypercholesterolemia, coronary heart disease, etc.
His grandmother had high blood pressure, but when asked whether the patient had any other diseases in the past, the patient and his family hesitated and did not say anything. The experienced emergency doctor thought that the patient had something unspeakable. , Secretly asked the patient, the patient said that he had been suffering from AIDS for 10 months, and he was currently taking icogen acetaminophen.
The disease progressed rapidly, the operator was informed that the patient had AIDS, and they were reminded to be safe, and the patient went to the emergency room for intervention.
Result report: no abnormality in the origin and course of coronary artery; right-dominant distribution of coronary artery; no obvious stenosis in left main (LM), distal blood flow TIMI grade 3; left anterior descending artery (LAD) segment stenosis 60%-70%, distal blood flow TIMI grade 3; left circumflex artery (LCX) with obvious stenosis, distal blood flow TIMI grade 3; right coronary artery (RCA) no obvious stenosis, distal blood flow TINI 3 grade; consider LAD borderline lesions.
Coronary flow reserve fraction test showed: 0.91, no stent implantation was given.

After surgery, patients were given aspirin, clopidogrel combined with antiplatelet therapy, atorvastatin to regulate lipids, metoprolol to control heart rate and reduce myocardial oxygen consumption.
On the second day, complete biochemical items, coagulation, slightly lower albumin, elevated myocardial enzymes, elevated alanine aminotransferase, aspartate aminotransferase, triglyceride and low-density lipoprotein, elevated electrolytes , uric acid, coagulation, etc. were not significantly abnormal.
Discussion
Myocardial infarction in young patients has associated risk factors, in addition to traditional risk factors such as smoking and dyslipidemia, coagulation-related genetic polymorphisms, fibrinogen, homocysteine It is related to new risk factors such as amino acid and uric acid [1], but this patient showed no obvious abnormality except for the related genes. It is not difficult to think that myocardial infarction in this patient is related to AIDS.
Main mechanisms of HIV infection predisposing to coronary heart disease:
HIV can affect blood lipid metabolism and can increase low-density lipoprotein cholesterol (LDL-C) and triglyceride (TG), which can lead to atherosclerosis.
HIV can induce endothelial dysfunction by activating protein kinases and leading to apoptosis of vascular endothelial cells.
HIV-infected people are chronically hypercoagulable, which increases the risk of coronary thrombosis.
Long-term antiretroviral therapy also increases the risk of coronary heart disease [2-6].
Clinical features of HIV infection complicated by coronary heart disease:
The clinical features of coronary heart disease in HIV-infected patients are similar to those in the general population, including quiescent myocardial ischemia, stable angina, and acute coronary syndrome< strong>. Acute coronary syndrome is often the first symptom in many patients.
HIV-infected patients show smaller lesions on coronary angiography than in the general population. The proportion of one-vessel disease is 35%-56%, the proportion of two-vessel disease is 18%-28%, and the proportion of three-vessel disease is 13%-76%.
After acute coronary syndrome in HIV-infected patients, 25%-76% received percutaneous coronary intervention (PCI), 4%-18% received coronary artery bypass 10%-20% received medical treatment.
HIV-infected patients with acute coronary syndrome have an in-hospital mortality rate of 0-8%.In-hospital heart failure and reinfarction rates did not differ from the general population; HIV-infected patients had higher rates of recurrent ischemic events during long-term follow-up than the general population, but cardiovascular mortality and overall mortality did not differ from the general population.
Efficacy of PCI after acute coronary syndrome in HIV-infected patientsSimilar to general population:
The incidence of short-term and long-term stent thrombosis after stenting is low and similar to that of the general population;
The incidence of restenosis after stenting is 9%-52%, which is similar to the general population;
Drug-eluting stents also reduce the incidence of stent restenosis in this population.
HIV-infected patients have a high incidence of coronary revascularization and re-myocardial infarction after acute coronary syndrome [2].
Prevention and treatment of coronary heart disease in HIV-infected patients: When treating AIDS patients, the risk of coronary heart disease and myocardial infarction in these patients should be taken into account. Come up with an overall plan.
First of all, these patients should be advised to change their lifestyles, such as quitting drugs, quitting smoking, increasing physical exercise, controlling blood pressure, changing bad eating habits, controlling blood sugar, and taking necessary lipid-lowering treatment, taking aspirin, etc. .
In anti-HIV therapy, the adverse effects of drugs on the incidence of coronary heart disease should be fully considered. On the premise of ensuring the efficacy, if protease inhibitors are not used, try not to use protease inhibitors; if protease inhibitors must be used, try to use drugs that have a low impact on the incidence of coronary heart disease, such as saquinavir [2] ].