Formerly on duty and worried about an orthopedic emergency, an appendicitis emergency, or a major car accident emergency. Today’s emergency room, “out of thin air” has an additional labor analgesia.

Faced with this new thing, many anesthesiologists have a lot of headaches. The reason is that I used to be confident in doing any anesthesia, and I really dare not challenge when it comes to labor analgesia.
Today, we will talk about this topic~
Let’s talk about labor analgesia first:
Labor pain relief, also called analgesic labor, is often referred to as “painless labor.” Generally speaking, “pain free” is just an idealized state. That is to say, medical staff can only reduce the pain during childbirth through various methods.
Currently, commonly used methods include psychoactive analgesia, acupuncture, transcutaneous electrical nerve stimulator, underwater delivery, analgesics, and spinal analgesia. . The specific implementation process can be refined into many forms such as prenatal education, family companionship, and doula delivery. In short, as long as the pain can be relieved, it belongs to the category of labor analgesia.

However, despite the many schools of thought, the only one that has been proven effective is neuraxial analgesia administered by anesthesiologists.
When obstetrics departments in various hospitals found that intraspinal analgesia was effective, they regarded intraspinal canal as a “magical skill”. When communicating with mothers, there is no reservation. As a result, the mother or family members think that “it won’t hurt if you hit it”. It is precisely because of this that the anesthesiology department is comparable to “riding a tiger” as soon as it appears. If it is not good, it seems that it is purely technical.

Today we will break it down: Is it technically poor, or is there another reason?
In essence, neuraxial analgesia is a nerve block. The key is whether it can be accurately blocked. If the pain reliever is blocking the target nerve exactly, there is no possibility of pain. Therefore, it is crucial to understand what nerve conduction is involved in labor pain.
Speaking of this, I believe it is also a knowledge point that many anesthesiologists care about. After all, this part of the anatomy is too detailed, and it may be a little vague or uncertain.
Labor pain is obviously related to the uterus, so let’s take a look at how the nerves of the uterus are distributed: the uterus is innervated by sympathetic and parasympathetic nerves, while the uterus and cervix are affected by different innervation.
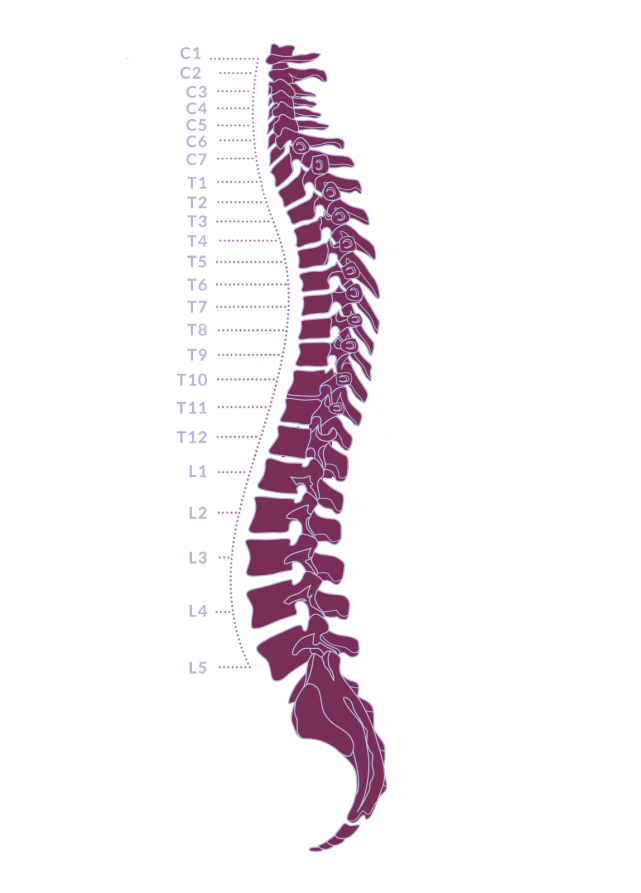
The movement of the uterus comes from the innervation of T5-T10 sympathetic motor fibers in the spinal cord. The preganglionic fibers exchange neurons in the adjacent sympathetic ganglia, and the postganglionic fibers participate in the formation of the pre-celiac aortic plexus. and the hypogastric plexus, which eventually form the pelvic nerve next to the cervix.
The sympathetic sensory fibers of the uterus pass through the pelvic plexus, hypogastric plexus, and aortic plexus into the lumbar and lower thoracic sympathetic trunks, and finally enter the spinal cord along the T11-L1 spinal nerves.
The movement and sensation of the cervix are mainly conducted by the S2~S4 parasympathetic nerves. On the sides and back of the uterus, the posterior branches join with the sympathetic nerves from the pelvic plexus to form the uterovaginal plexus and cervical nerve. Sensation in the upper part of the vagina is conducted by the S4 parasympathetic nerve, and the lower part of the vagina is composed of the anterior branches of the S2-S4 spinal nerves.
Obviously, a good labor analgesia should control pain through T10-S4 nerve conduction. However, the best block range for intraspinal analgesia is the three segments above and below where the catheter tip is located. And T10 ~ S4 exactly six segments. That is, the catheter tip should be placed exactly at the midpoint of L1.

The question is: who can put it so accurately?
If you are not an anesthesiologist, you may not understand what this means.think. This is related to the operation of spinal canal puncture: spinal canal puncture is a blind detection operation. Although some hospitals currently use ultrasound guidance, they are very few. Blind detection operation may be inaccurate. Another objective reason is that the positioning of the puncture point is completely based on the feel, and this error is completely forgivable if it is within a segment.
However, labor analgesia does not give you the chance to miss a segment. Therefore, some of the incomplete block is also objectively unavoidable.
Some people say that it was fine at first, but then it hurts badly.
About this, it has to do with labor. The first stage of labor is mainly T10 ~ L1 conduction of uterine contraction pain.
The pain at this time is usually higher in the stomach. If the catheter is just inclined to a high place, it should not be painful, or the pain will improve significantly.
However, once the second stage of labor is reached, the pain relief is not sufficient. Because, the pain in the second stage of labor is mainly the pain caused by the compression of the fetal presentation conducted by S2~S4.
At this point, increasing the dose may not help.
At this time, if the mother cannot tolerate pain, has large mood swings, or the fetus itself is somewhat hypoxic, it is very likely that abnormal fetal heartbeat will occur. Because of this, this process often becomes a high-incidence period of natural birth failure.
At this point, my sharp-eyed friends seem to have noticed the word “emotion”. Is Pain Also Emotional?
Of course it does, and it does matter a lot.
Let’s look at the definition of pain: It is an unpleasant feeling, and emotional experience, associated with tissue damage, or potential tissue damage, or similar damage as described.

To put it bluntly, it is as much pain as you feel.
If you still don’t understand, here’s an example: Suppose a person sings in a dance hall and accidentally gets scratched by a wine bottle, he will not feel too much pain. At that time, because he was very excited, his focus was not on the wound; for another example, if a soldier was charging, would he be sensitive to pain? No, because he’s focused on fighting.
So what we’re saying is, learn to be distracted. In practice, it has been found that those who cry out in pain and can’t hold on to the transfer are usually afraid of pain. The reason for this is that he is too focused on having children.
In conclusion, don’t take labor pain relief so seriously. The higher the expectation, the worse it is, and it should be treated with normality. As long as the pain is relieved a little, it is already happier than before. If the effect is very good, it means that the anesthesiologist is accurate and you are well adjusted.
[Warm reminder] Please pay attention, here are a lot of professional medical science, to reveal the secrets of surgical anesthesia for you~