When “adenoid hypertrophy” is mentioned, many people think of mouth breathing, snoring, becoming ugly, and seriously causing brain damage. Research shows that at least 3 out of 10 children have adenoid hypertrophy. The backstage of lilac mother often receives related inquiries, such as:
The child continues to snore, mouth breathing, and wakes up frequently at night. Is it “adenoid hypertrophy”?
Conservative treatment or direct excision for the child’s “adenoid hypertrophy”?
Can I not remove it and wait for my child’s adenoids to shrink on their own?
Is the surgery OK? are there any side effects?
In what circumstances must it be cut, and what will happen if it is not?
……
The protagonist of today’s story shared that her baby went from being diagnosed with “adenoid hypertrophy” to conservative treatment. Because there was no timely surgery, it also caused otitis media. She suffered a lot and finally had her adenoids removed. detailed experience.
Surgery is not terrible, but blindly resisting surgery delays the disease. I hope today’s sharing can give you some reference and help.
This article is from lilac mom APP planet @Di Mom Complementary Food Notes
The adenoidectomy surgery, I regret doing it late, I have been hesitant to delay it for more than a year, and the child has suffered a lot.
Rhinitis has been bad
Mouth breathing and snoring also occur
Back in time two years ago, 2-year-old Andy always rubbed and picked his nose, and sometimes had nosebleeds.
At that time, I went to the hospital for treatment. The doctor said it was dry rhinitis, and prescribed sea salt spray and hospital-made nasal drops. I didn’t think it was serious at the time, and Andy had been uncooperative, so I always took the medicine for three days to fish and two days to dry the net.
In this way, Andy’s symptoms have not been relieved, and there have been restless nights and frequent night awakenings.
When I was about 3 years old, I noticed that Andy also started snoring in sleep and mouth breathing.

Image source: Courtesy of the author
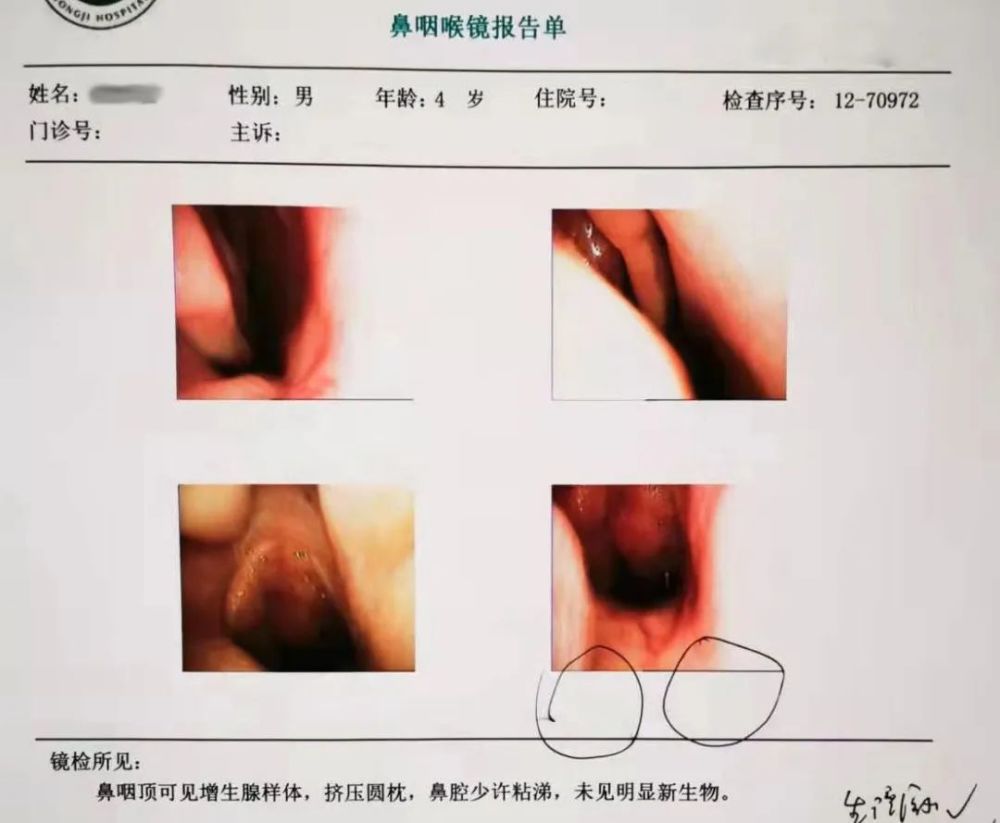
During that time, I happened to see an article on the Internet on popular science about “adenomatous hypertrophy”. At that time, I felt very similar symptoms, so I quickly changed to another hospital and went to the otolaryngology department for a re-examination.
Because Andy did not cooperate with the nasopharyngoscopy examination, the doctor asked Andy to do a lateral nasopharyngeal examination. This examination was a bit radiant, but not painful, and the child was very cooperative. It is relatively high, but the result may be inaccurate due to the child’s tampering.
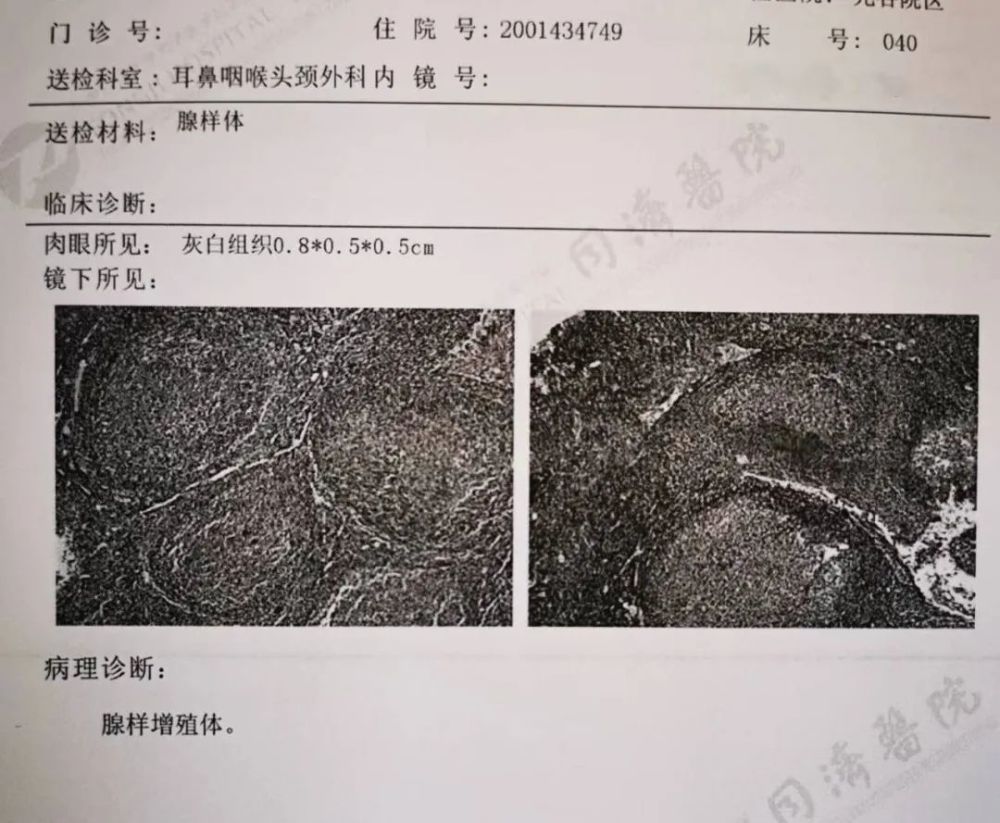
The results showed that Andy’s A/N ratio for Adenoid Hypertrophy was 0.68.
When the doctor saw the lateral view of the nasopharynx, the doctor initially judged that the A/N ratio was 0.8, which was pathological hypertrophy. After repeated confirmation with the doctor who took the film, the A/N ratio was determined. is 0.68.

Image source: Courtesy of the author
The doctor said that the A/N ratio between 0.61 and 0.70 is moderate hypertrophy, and the A/N ratio above 0.71 is pathological hypertrophy, and there are clinical symptoms such as persistent snoring or mouth breathing, and repeated rhinitis. When symptoms are present, general anesthesia surgery is recommended.
Although Andy’s current blockage is not particularly serious, but there has been rhinitis and unsteady sleep. Conservative treatment can be performed first, and then decide whether to surgery or not. .
I immediately checked some information on the Internet and said:
Adenoids are immune organs composed of some lymphoid tissues. The reason for hypertrophy is caused by factors such as inflammation. Repeated stimulation of adenoid hyperplasia can lead to nasal congestion, snoring, and mouth opening. Breathing, apnea, etc., may also lead to “adenoid face”.
Hypertrophic adenoids squeeze the Eustachian tube, and otitis media may also occur, causing hearing loss; sleep apnea syndrome, cerebral hypoxia, and the risk of mental decline.
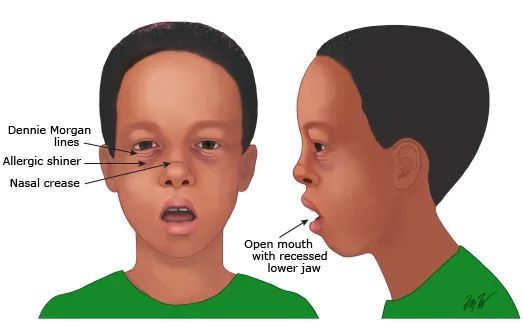
Adenoid face, photo credit: UTD
I was nervous for a while, but then I saw:
Adenoids develop from the age of 2 and are divided into physiological hypertrophy and pathological hypertrophy. Physiological hypertrophy will mature in immune function and gradually shrink after about 10 years of age, almost invisible to adults.
I immediately began to feel fortunate again, and lamented that it was fortunate that Andy found it early and had not developed pathological hypertrophy, so he could be treated conservatively first.
I made up my mind that I must follow the doctor’s orders and cooperate with the treatment at home so that Andy would not have to undergo general anesthesia.
The doctor prescribed us the nasal steroids Nessana, Montelukast Sodium (Singularin), Sea Salt Water, and Cetirizine:

Image source: Courtesy of the author
Sea salt water is used for daily nose cleaning, 2-5 times a day;
Cetirizine is an antihistamine, 5 mg every night;
Nexona, chemical name mometasone furoate, is a nasal spray hormone, the first choice for the treatment of allergic rhinitis, once a day;
Montelukast sodium, trade name Singulin, can inhibit the proliferation of adenoid lymphocytes and is effective for mild to moderate adenoid hypertrophy.
This is how we began the long road to conservative treatment.
Repeatedly ill, often waking up from sleep
Finally made up my mind to have surgery
At first, under the control of drugs, Andy’s condition did improve, and he could observe that his sleep was slightly better, and his mouth breathing was also relieved.
However, It is frustrating that the condition keeps coming back and forth. I often feel relieved and start to get nervous again. At first, my child seems to be getting better. Been in awe all day long.
In addition, due to poor sleep, Andy’s growth and development is not good, and his height and weight are a little behind children of the same age. Immunity is also poor, frequent sickness, runny nose, coughing.
In short, during that time, the whole family followed the child’s condition, and it was like a roller coaster.

Image source: Zhanku Hailuo
After 8 months of conservative treatment, Andy’s condition was getting worse, and he was waking up frequently and crying constantly at night.
I checked the Internet and found that it may be caused by apnea caused by “adenoid hypertrophy”. Apnea is likely to cause hypoxia throughout the body, and even affect the child’s brain development and intelligence.
I started thinking about surgery, but was hesitant.
On the one hand, I feel that it is “general anesthesia surgery” after all. I have absolutely no idea what risks such a young child will face, whether there will be psychological shadows, etc.
On the other hand, I am afraid that Andy will have an “adenoid face”, and I am worried that repeated illness and apnea will have a worse impact on the child.
During such hesitation, we took our children to see all the hospitals in Wuhan. Some doctors suggested doing it, some doctors didn’t recommend doing it, and some doctors suggested cutting the “adenoids” separately. Some doctors suggested that the “tonsils” be cut together.
In short, after a look around, it’s even more tangled.
So, I started frantically looking up information on the Internet, bought a lot of courses related to “rhinitis” and “adenoids”, and also asked my friends and various mothers if there were any children who did it. After “adenoidectomy”, which doctor and which doctor did it well, how was the recovery after surgery, how was the effect of the follow-up surgery, etc.
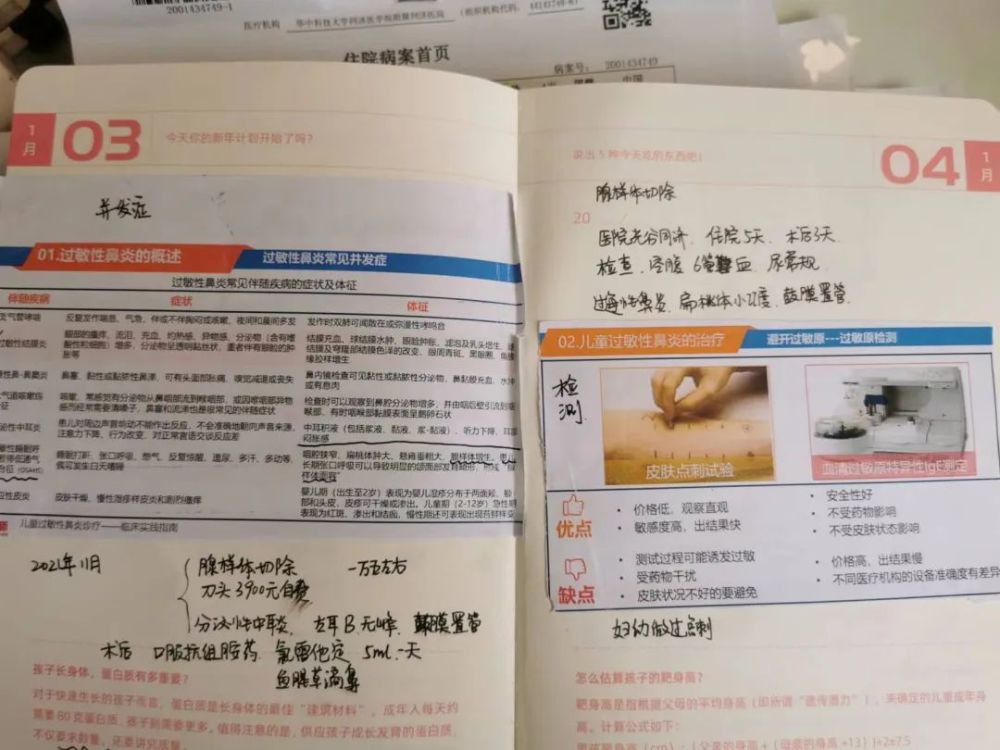
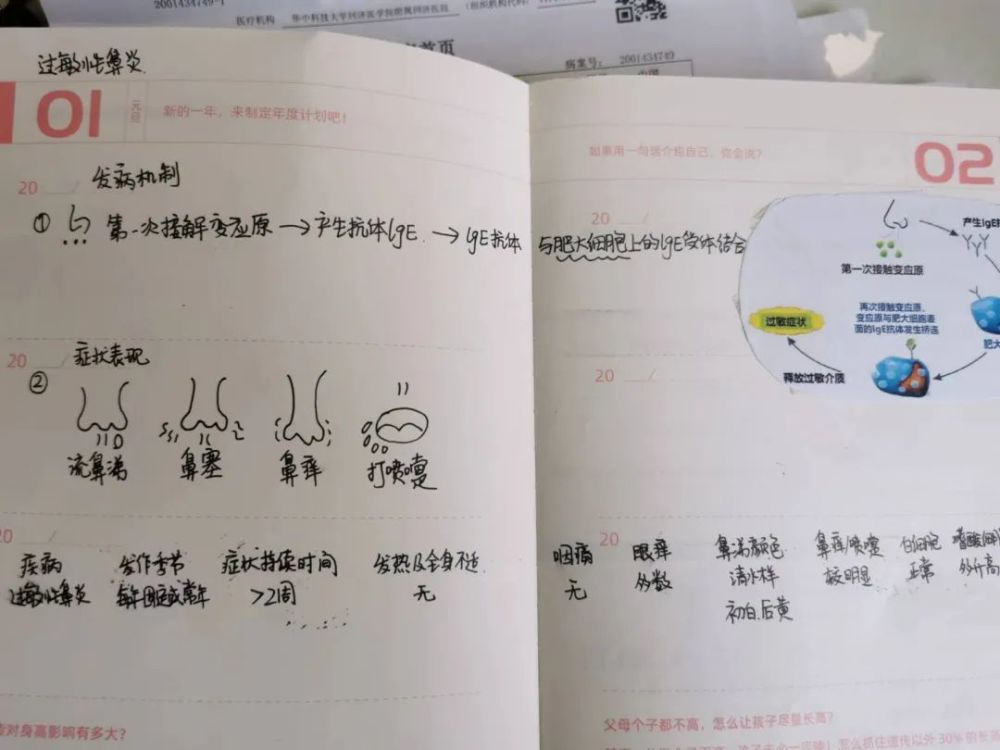
Swipe left to see more, image source: courtesy of the author
Although I learned that “Adenoidectomy” is only a minor operation, the child will not be too uncomfortable, and the postoperative improvement is generally good. But when it came to my child, I was still apprehensive and hesitant.
Until Andy got sick again. This time, due to bad rhinitis, constant coughing, and frequent waking up and crying at night, Andy suffered for more than a month.
Seeing that the child was so uncomfortable and couldn’t sleep well at night, we finally made up our minds to have surgery.
Otitis media discovered before surgery
Lack of timely treatment affects hearing
Once we decided to have surgery, we hurriedly made an appointment with the doctor and started various pre-hospital preparations.
Among them, I pay the most attention to the child’s psychological condition, and I am afraid that he will have a bad shadow due to the operation.
I bought some picture books and told him how human beings were defeated by the bacteria king, and how the immune guards in the body defeated bacteria; I also specially found some 3D animation videos of surgery for children Look; I also shared my experience of having surgery when I was a child to my children, and let them accept the surgery little by little.

Swipe left to view, image source: courtesy of the author
We have been waiting over a month for surgery due to the pandemic.
As I remember well, we were admitted to the hospital on October 22, 2021. The day before the operation, Andy did various detailed preoperative examinations, including blood routine, urine routine, acoustic impedance, hearing examination, electrocardiogram, and lung CT.

Image source: Courtesy of the author
It was only then that we discovered that Andy’s “hypertrophic adenoids” also caused secretory otitis media, with fluid buildup in the left ear and invagination of the tympanic membrane.
Combined with the hearing test at the time, the doctor suggested that we do a catheter placement, saying that if it is not treated in time, it will cause irreversible effects on hearing.
I was stunned for a while. I didn’t expect “adenoid hypertrophy” to affect hearing.
Annoyance and self-blame flooded into my head, regretting why I dragged the child like this, so I decided to operate.
Swipe left to see more, image source: courtesy of the author
On this day, the doctor also had a detailed preoperative communication with us.
The doctor said that general anesthesia is injected according to the child’s weight, and the anesthesiologist will confirm the child’s weight with us. General anesthesia will generally not affect the child.
We chose low temperature plasma ablation for the surgery. Compared with the ordinary excision surgery covered by medical insurance, although this surgery is self-paid and more expensive, it is more traumatic to the surrounding tissue. Small, less bleeding, and the child is more comfortable.
Doctors also say there is a risk of recurrence after surgery, hypertrophic adenoids andEnlarged tonsils can lead to poor breathing and snoring. If the adenoids are removed alone, there may be a risk of a second removal of the tonsils.
The chief surgeon recommends removing the tonsils together, which can better solve the problem of snoring and mouth breathing in children.
But considering the difficulty of postoperative care and Andy’s cooperation, I still want to keep the tonsils first, and accept the risk of a second operation. At my insistence, the doctor had to agree to my request.
In addition, regarding the child’s otitis media, the doctor recommends placing a tympanic membrane tube directly during the operation. I’m hesitant to do this or not, I didn’t know it at all before.
I searched the Internet and found out:
Adenoid hypertrophy can lead to a blockage of the Eustachian tube or passage of pathogens through the Eustachian tube into the middle ear, resulting in otitis media.
Otitis media is divided into secretory otitis media and acute otitis media. Most secretory otitis media is mainly manifested by hearing loss, but young children do not recognize hearing impairment, so it is usually hidden and difficult to detect. Diagnosis can be made by otoscopy.
After discussing with my teammates, I finally decided to perform tympanic tube surgery at the same time as the adenoidectomy. At that time, I thought that I would also have a general anesthesia surgery, but I was still very nervous, I am not sure if my decision was right.
Andy has been very nervous all day, and he is also restless at night. He always wakes up in the middle of the night and says that my mother is afraid and wants me to hold her.
We were huddled together in the hospital ward, but our hearts were very close. The little he I can feel needs me especially at this moment, I gently stroke him, soothe him until he falls asleep again.
21 hours without food or drink
Son crying for meat
Andy was placed third on the day of the surgery.
Because of the fasting of food and drink before the operation, Andy had not eaten or drank from 9 o’clock in the evening until 11 o’clock the night before. said to me that he wanted to eat.
While waiting, in order to relieve tension, I took out a specially prepared toy to play with Andy.
Image source: Courtesy of the author
Finally made it to the operating room where my husband and I waited anxiously outside. The waiting area was crowded with people coming and going, and we were staring at the lobby screen.
Even though I knew it was a minor operation, I was still nervous. I resisted and sat still, feeling every second extraordinarily long.

Image source: Courtesy of the author
The surgery took more than an hour, and the rest was waiting for the anesthesia to come out.
As soon as I heard his cry, my tears finally couldn’t hold back. I felt that nothing was important at the moment. I ran to the operating room, and the moment I saw Andy, a The heart that was hanging in the air finally fell to the ground.
Andy was lying on the hospital bed. Maybe the anesthesia was not over, and he was a little dizzy. He cried immediately when he saw me. I hugged him for a while and fell asleep.

Image source: Courtesy of the author
After the operation, the doctor told me to continue fasting for 4 hours. After waking up, the little guy was so hungry that he kept crying and kept shouting, “Mom, I’m hungry, I to eat meat.”
After the operation, Andy had no fever, no pain, no vomiting blood. He was in much better condition than the children who had their tonsils removed in the same ward, and could eat some liquid food.
We stayed in the hospital for 3 more days and the doctor saw the baby was in good shape and was discharged.

Eating noodles after surgery, image source: Courtesy of the author
Surgery works well
Regret not having surgery earlier
After I got home, I followed the doctor’s advice and took good care at home for a period of time, and I stopped all classes of strenuous exercise (tympanic tube can not be strenuous exercise). Di eats liquid food.
Surgery works really well. Andy’s sleep has improved a lot, his breathing is smoother, the snoring has gradually disappeared, and he has never been woken up again, and he can finally sleep soundly.
Listening to his smooth breathing and looking at his sleeping face, it feels like a battle has come to an end, I’m really relieved, and I regret always being afraid of children Suffering, he didn’t do the surgery early, but invisibly made him suffer more.
Especially after conservative treatment did not improve for 8 months, there was still hesitation and delay for a while.

Image source: Courtesy of the author
Looking back now, I think everything is very clear. It really shouldn’t delay the child for so long. The child is uncomfortable and the parents are also suffering. But at that time, I really hoped that I could not do the surgery without general anesthesia, not to mention that the doctor also recommended conservative treatment first.
Of course, not all hypertrophic adenoids require surgery. Looking back on the whole process of taking Andy to see a doctor, I finally share with you all:
1.Hypertrophy of adenoids may cause otitis media, do not ignore this, observe the child’s speech response, do otoscopy and acoustic impedance to check whether there is Otitis media and hearing loss.
About whether otitis media should be intubated or not, I checked some information later, found that when the course of unilateral or bilateral secretory otitis media is more than 3 months, the tympanogram is C-type Or type B, tympanic membrane tube placement is only required if one of the following conditions is present:
Hearing loss ≥ 25 dB HL with poor air conduction or impairing speech learning and communication;
Introduction, adhesion, or effusion of the tympanic membrane was found on examination;
≥3 episodes in 6 months, or ≥4 episodes in 1 year.
Don’t be like us at the time, making decisions in a panic because time is too tight to inquire.
2. When the child is rubbing the nose, stuffed, runny, sneezing< /strong>, please pay attention. If the child has allergic rhinitis, repeated stimulation of rhinitis will cause adenoid hyperplasia. If the rhinitis is diagnosed, the child can be taken to the ENT department for further examination;
3. Adenoid hypertrophy surgery cannot eradicate allergic rhinitis. Do not believe in moxibustion and nose fumigation. Scientific and evidence-based treatment is required. Allergic rhinitis should be controlled after operation. It is very important to choose isotonic sea salt water for daily cleaning of the nasal cavity.
4. Not all hypertrophic adenoids need to be removed, but when the following situations occur, don’t hesitate, just do it, the longer the delay, the more harm will outweigh the benefits:< /p>
Presence of moderate nasal obstruction with mouth breathing, obstructive nasal sound, or anosmia persisting for at least 1 year and not responding to conservative treatment;
Recurrent upper respiratory tract infections, epistaxis, nasal or sinus inflammation;
Adenoid facies developed.
5. When the child has apnea or wheezing at night, or sleeps “unrestful”, you can go to the hospital to monitor the child’s sleep condition through “polysomnography” to determine whether there is severe Obstructive sleep apnea, from this to see whether “adenoidectomy surgery” is necessary.
Andy did not do this test at the time because of other clinical symptoms that were judged to be surgery.
Okay, the above is the real experience of taking my baby to do “adenoidectomy”. If your baby or friends around you have also experienced adenoid hypertrophy, welcome to leave a message area comminicate.
If you find this article useful, remember to forward it to your friends and give them some reference!
References
[1] Stephen I Pelton,MD,Tal Marom, MD,Otitis media with effusion (serous otitis media) in children: Management.UpToDate
[2] llen R Wald, MD.Tonsillectomy and/or adenoidectomy in children: Indications and contraindications.UpToDate
[3] Guidelines for the diagnosis and treatment of secretory otitis media in children ( 2021 ). Chinese Journal of Otolaryngology Head and Neck Surgery. 2021.56(6)
This article expert

Pan Chunchen

Review Specialist
The First Affiliated Hospital of University of Science and Technology of China, Otolaryngology
Deputy Chief Physician of Head and Neck Surgery
Fan Yunzhu
Review Specialist
Lilac Clinic Pediatric Attending Physician
Planning
Planning: Lin Yiyi
Producer: Astro
Typesetting: Lin Yiyi
The source of the title map: Zhanku Hailuo
This article is from lilac mom APP planet @Di Mom Complementary Food Notes