Author, Shuli Sun
Unit: Tangshan Nanhu Hospital, Tangshan City, Hebei Province
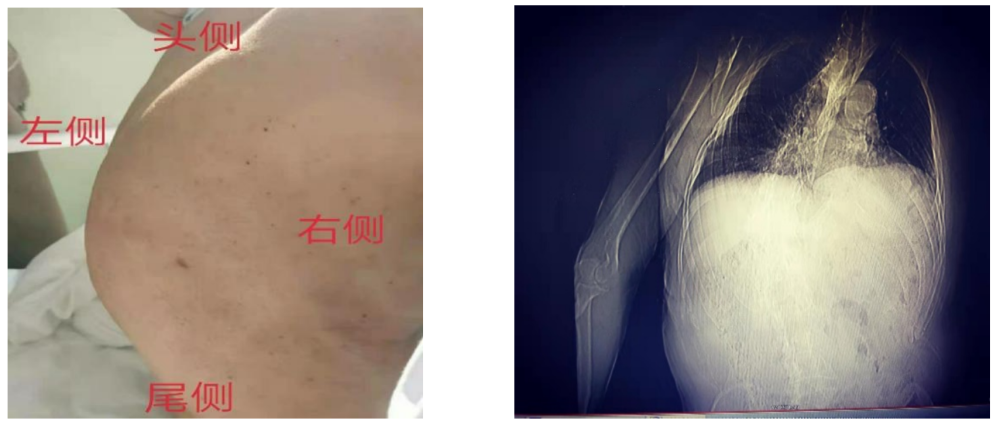
The patient, an 80-year-old male, was admitted to the hospital mainly due to progressive dysuria for 8 years and was diagnosed with benign prostatic hyperplasia. After admission, the examination revealed that the thoracic spine was extremely rightward, unable to lie down, and hearing was extremely poor. Cardiac function grade III, ground-glass nodules in the upper lobe of the right lung, and symptomatic changes in the left and lower right lungs. 10 years after brain tumor surgery, 7 years of history of hypertensive cerebral infarction, unfavorable right lower extremity activity, and the current blood pressure control is acceptable.
In view of the patient’s current medical condition, a plasma resection of the prostate is planned. Therefore, our department recommends to adjust the cardiopulmonary function first, and then perform surgery after the cardiopulmonary function improves and stabilizes. Otherwise, a patient with such a bad general condition will not recover well after the double blow of surgery and anesthesia.
However, the director of the urology department has already patted the chest with the family, saying that the operation is not complicated and will not take too long. It’s true that the surgeon only treats the disease! As long as we have one-third of our own land, this problem is left to our anesthesiology department.
After discussion in the department, in order to reduce respiratory complications after general anesthesia, reduce the impact of general anesthesia on cardiopulmonary function and general condition, as well as the patient’s position problem. Spinal anesthesia is the first choice, and general anesthesia is the alternative.
Friday afternoon, when I was about to get off work, the director assigned me to the ward for a pre-operative visit and an ultrasound to evaluate the spinal condition. So, I hurried to the ward with the color Doppler.
At that time, I analyzed that it was not me who did this anesthesia. Reasons: my surgery wasn’t done yet, and my colleagues took care of me; Corey still had some unfinished business; I happened to be off the night shift on Monday. If the night shift continues the operation, I am afraid that the anesthesia on Monday morning may also be exhausted and not enough energy. So the chances of this anesthesia for me are not too great.
I went to the urology department to see the doctor in charge. After a brief introduction to my condition, he kindly reminded me that this patient is a super VIP with a special background and is highly valued by the leaders of our hospital. Relatively high, we must pay attention to the way of communication.
The kind reminder from the doctor in charge, today when the doctor-patient relationship is so tense, I remind myself: I must be kind, communicate well with the patient’s family, and gain the understanding and trust of the family. .
Walking into the ward, I saw the patient in a semi-recumbent position, with steady breathing, complaining of shortness of breath after activity, and coughing with a small amount of white sputum.
Explain the purpose of the visit to the family members, and after a simple and friendly communication, ask the patient to evaluate the spinal condition in the lateral recumbent position.
Because the elderly have extremely poor hearing, indwelling urinary catheters, inconvenient activities, and their family members do not actively cooperate, it takes a lot of effort to change the body position.
With everyone reaching out and supporting me, I used a color Doppler to scan the transverse and sagittal planes of the lumbar spine, and then hurried back to Corey.

On Saturday, the director suddenly sent me a message saying that we all remember to take pictures of the patients undergoing resection of the prostate in the urology department on Monday, and keep first-hand materials.
I didn’t realize at the time that the anesthesia was going to be my responsibility and I was lucky. I thought about the special patients I met before, whether it was for study or for publicity, I also left photos.
In less than 5 minutes, the director said in the department group that I will perform the anesthesia in person and ask everyone to come and watch.
My head was buzzing and I felt a lot of pressure! First, it is estimated that the puncture is very difficult, there is uncertainty about whether the puncture can be successful, and whether the spinal anesthesia can be successfully implemented, I am not fully sure. Second, I am reluctant to do this kind of anesthesia for VIP patients, and the reasons are self-evident.
Since the director has arranged this, I have no good reason to refuse it! It means that the director still trusts me very much, so let’s rise to the challenge!
It was Monday morning, and after the shift was over, the patient was taken to the operating room on time. I have all the narcotics ready.
Open the vein, monitor the oxygen, and help the patient to position. I thought that this time I must use ultrasound to evaluate the patient’s spine, make a puncture location, measure the distance from the skin to the subarachnoid space, and even puncture under the guidance of ultrasound.
After positioning, the patient’s spinal deformity seems to be more severe – the entire spine is not in a straight line at all, showing a large “S” shape. And the thoracic spine protrudes to the right and posterior, reaching the level of the right subscapular angle, the anterior and posterior diameters > the left and right diameters, and the lumbar spine curves to the left ventral side.
Seeing that all my colleagues came to watch, I repeatedly persuaded me, but no one left. This has increased my psychological burden even more, I’m afraid there is no place to put it if I can’t get it on my face!
After starting the operation, I first scanned the lumbar intervertebral space with ultrasound, and repeatedly scanned the intervertebral space between the lumbar 1 and 4, but there was no anterior complex, only the space between the lumbar 4 and the 5 was vaguely visible. thing. Measured the depth of the subarachnoid space at about 4.8cm, which gave me a little more confidence.
Historically, as long as the anterior complex is visible on ultrasound, the chances of a successful puncture are very high. Because the anterior complex includes the medial dura mater, connective tissue, the posterior longitudinal ligament, and the vertebral bodies and intervertebral discssome organizations. These tissues can be seen, indicating that there is no obstruction on the puncture path, ultrasound can be transmitted, and of course the puncture needle can pass through.
Disinfect the drape and start the operation. I meditate in my heart: I am “Sun Yizhen” from the Department of Anesthesiology of Nanhu Hospital, I must show the domineering spirit of Nanyi people, only success, not failure, come on! come on! come on! At the same time, I was thinking: If I can’t get on, who will be my “Panman”? I used to be someone else’s “catchman”!
It is better to believe in yourself than to believe in others. Dreaming can’t solve the problem, so let’s do it first! Based on the information provided to me by ultrasound and my previous puncture experience, I decided to choose subarachnoid puncture first, and then choose combined spinal-epidural puncture in case of failure.
Because the patient is 80 years old, the lumbar ligaments are likely to be calcified, and the range of motion of the vertebral joints is poor. I thought that the needle insertion point must be selected, whether it is straight or side entry. Of course, the needle insertion path is also very important.

Because my colleagues were all watching, I was still a little nervous, took a deep breath, calmed down a little, followed the ultrasound positioning, and began to insert the needle based on experience and feel. With my thrust slowly into the patient’s body. The resistance was a little large, and soon the needle tip touched the bone, and the first needle insertion failed. Withdraw the needle under the skin, prepare to change direction, and insert the needle again.
At this time, fine beads of sweat were oozing from my forehead, and my hands were shaking. However, I kept telling myself to keep calm! calm down! Calm down!
After adjusting the direction and inserting the needle again, the bone was not touched, and the resistance of needle insertion suddenly decreased, and I felt a sense of disappointment. Visual inspection of the depth of needle insertion was close to the value measured by ultrasound. I thought to myself that it should enter the subarachnoid space, and it should not be far from success. I carefully pulled out the needle core, looked sideways at the needle end, and the colorless and transparent cerebrospinal fluid slowly flowed out.

At this moment, I barely suppressed my inner ecstasy, raised my right hand, and made an OK gesture to everyone. Colleagues also gave thumbs up. If the patient is not awake at this time, I think I will jump up and cheer with everyone. In an instant, the flashes of my colleagues’ mobile phones continued to light up, and it really felt like they had won the world championship.
After a successful subarachnoid puncture, the cerebrospinal fluid returned smoothly. Given that the patient’s spine is extremely curved to the right and rear, a semi-recumbent position is required at an angle of about 30 to 40 degrees with the bed, the spinal canal may be bent and stenotic, and the cardiopulmonary function is so poor, the anesthesia level can be satisfied at T10 Require. I put the opening of the needle tip toward the head, and slowly (30s) injected 2ml of ropivacaine (1% ropivacaine + 10% glucose 1ml).
After turning over and lying down for 5 minutes, the T10 level of the anesthesia plane was measured. The operation started with satisfactory anesthesia effect.
In order to relieve the patient’s nervousness and spend a comfortable period of operation, sedatives were pumped and the patient could sleep peacefully.
The operation lasted for 50 minutes. After the operation, the patient’s name was called out through the ear, and the eyes were opened immediately, so that he could communicate with everyone normally. He told him that the operation was over, asked him if it was painful, and said with a smile, “I don’t know if the operation is over, and gave me a thumbs up at the same time.”
This case tells us that we should not only have a wealth of theoretical knowledge, but also make a thorough anesthesia plan according to the different conditions of each patient, but also have skilled operation techniques. Despise the enemy strategically and pay attention to the enemy tactically. Not to forget our third eye – ultrasound.
The advantages of ultrasound visualization are self-evident, it can not only accurately locate and guide us in the direction of various punctures, but also greatly improve our puncture success rate. Without the reliable information that ultrasound provides us with this patient, the puncture probably would not have been successful, or even so easily. Once the puncture is unsuccessful, it is bound to switch to general anesthesia to complete the operation. I believe there is no need for me to say more about the adverse effects of general anesthesia on the patient.
Suppose you encountered such a case, how would you choose? Welcome to leave a message and exchange~
[Warm reminder] Please pay attention, here are a lot of professional medical science, to decipher those things about surgical anesthesia for you~