*For medical professionals only
6 classic prescriptions to explain the rational use of hypertension!
As we all know, hypertensive patients often have many clinical complications, so the phenomenon of combined medication is very common, and the most important thing that cannot be ignored is the drug interaction and the complications of the patients.
So, in clinical work, have you ever stepped on the pit of your combination drug prescription? The following is the author’s summary of 6 cases of irrational drug prescriptions for patients with typical hypertension. Let’s take a look!
Case 1
(1) Patient information: male, 55 years old.
(2) Clinical diagnosis: bilateral renal artery stenosis, secondary hypertension.
(3) Prescription medication:
(4) The analysis is as follows:
Enalapril maleate is not suitable:
Bilateral renal artery stenosis is a contraindication to angiotensin-converting enzyme inhibitor (ACEI) [2]; calcium antagonist (CCB) or beta-receptor antagonist is recommended.
Amlodipine besylate combined with simvastatin (metabolized by CYP3A4) increases the risk of rhabdomyolysis:
Simvastatin and amlodipine are substrates of CYP3A4, and their combined use will increase the plasma concentration of simvastatin. If combined use is required, the dose of simvastatin should be limited to Below 20mg/d.
Physicians and pharmacists should explain to patients:
In the event of unexplained muscle pain, weakness, or cramping, immediate medical attention should be sought, and other drugs such as pravastatin (which are not metabolized by P450 enzymes) are recommended.
Case 2
(1) Patient information: female, 60 years old.
(2) Clinical diagnosis: hypertension with severe liver damage.
(3) Prescription medication:
(4) The analysis is as follows:
Telmisartan is not suitable:
Telmisartan is mainly excreted through the bile, and patients with biliary obstructive disease or hepatic insufficiency may lead to reduced drug clearance of telmisartan, resulting in severe liver damage, cirrhosis Angiotensin II receptor antagonists (ARBs) are contraindicated in patients with biliary tract obstruction, and patients with mild to moderate hepatic insufficiency should be used with caution in dose adjustment [3]. It is recommended to choose ACEI/CCB with little effect on liver excretion/metabolism (the selection of drugs is not suitable).
Case 3
(1) Patient information: Female, 58 years old.
(2) Clinical diagnosis: hypertension grade 3 (very high risk), type 2 diabetes, diabetic nephropathy, chronic kidney disease (CKD) stage 4
(3) Prescription medication:
(4) The analysis is as follows:
Hydrochlorothiazide is unreasonable:
In patients with chronic kidney disease (CKD) stage 4, renal function is severely impaired. The main site of action of hydrochlorothiazide diuretics is the epithelial cells of the distal convoluted tubule. The filtration rate is significantly reduced, resulting in a significant reduction in the amount of drug reaching the site of action without the corresponding effect. Hydrochlorothiazide is contraindicated for glomerular filtration rate [4]. The loop diuretic furosemide is recommended.
The choice of captopril is unreasonable:
Captopril is a short-acting antihypertensive drug. Hypertension guidelines recommend choosing a long-acting antihypertensive drug as much as possible. ACEI/ARB drugs have antihypertensive effects, can also reduce proteinuria, delay the decline of renal function, and improve the renal prognosis of CKD patients [5]. However, if the serum creatinine level is > 265 μmol/L, or the glomerular filtration rate is lower than 30 ml/min, ACEI should be used with caution or disabled. Fossinple [6].
Therefore, it is not suitable for patients with chronic kidney disease (CKD) stage 4 to choose captopril.
Case 4
(1) Patient information: Female, 60 years old, with repeated heart palpitations, shortness of breath, blood pressure 180/90mmHg.
(2) Clinical diagnosis: hypertension grade 3 (very high risk), hypertensive heart disease, left ventricular ejection fraction (LVEF) 32%, cardiac function grade IV.
(3) Prescription medication:
(4) The analysis is as follows:
It is unreasonable to choose CCB nifedipine:
CCB drugs have no obvious beneficial effect on cardiac function and clinical outcomes in patients with heart failure. When diuretics are used in combination with ACEI/ARB and beta-blockers and/or aldosterone Blood pressure remains higher than 130/80 mmhg in patients with hypertension and heart failure after steroid antagonists, or in patients with heart failureWhen combined with angina pectoris, long-acting dihydropyridine CCBs (amlodipine or felodipine) can be given.
Among the calcium antagonists, only amlodipine and felodipine had a neutral effect on mortality in patients with cardiac insufficiency. CCB drugs such as nifedipine, verapamil or diltiazem have obvious negative inotropic effects and should be avoided in hypertensive patients with left ventricular systolic dysfunction. The patient is advised to choose amlodipine or felodipine.
Irregular treatment regimen, no diuretics:
The patient was diagnosed with hypertensive heart disease, LVEF 32%, and cardiac function class IV. Repeated palpitations, shortness of breath heart failure attack, given anti-heart failure treatment. According to the guidelines for the diagnosis and treatment of heart failure, diuretics act rapidly and can take effect within a few hours or days. Their effects on reducing blood volume and eliminating edema are better than any other anti-heart failure drugs. Diuretics are only suitable for fluids. Retention and symptomatic heart failure [7].
Patients with grade IV cardiac function should be treated with spironolactone, an aldosterone receptor antagonist, on the basis of diuretics. It is recommended that the patient be treated with furosemide, which can be used both intravenously and orally at the same time. After the symptoms improve, oral treatment is given, and spironolactone is combined at the same time.
Case 5
(1) Patient information: Female, 33 years old, blood pressure 175/115mmHg.
(2) Clinical diagnosis: 2 pregnancies, 1 intrauterine pregnancy, 32 weeks single live birth LOA, gestational hypertension
(3) Prescription medication:
(4) The analysis is as follows:
The patient was diagnosed with gestational hypertension, and it was unreasonable to give captopril tablets:
Captopril is a competitive angiotensin-converting enzyme inhibitor, and the U.S. Food and Drug Administration (FDA) classifies the pregnancy safety of captopril as C (first trimester) ) and D grades (second and third trimesters). The use of captopril in the second and third trimesters of pregnancy can lead to fetal death or damage to the neonatal renal system, fetal lung dysplasia, skeletal deformities, and even neonatal death.
According to the guidelines for rational use of hypertension [8]: the most commonly used oral drugs for gestational hypertension are labetalol, methyldopa and nifedipine, and low-dose thiophene can be considered if necessary Zine diuretics; ACEIs and ARBs are contraindicated during pregnancy, and should also be discontinued in patients with chronic hypertension who plan to become pregnant.
Case 6
(1) Patient information: female, 68 years old, blood pressure 170/95mmHg.
(2) Clinical diagnosis: coronary heart disease, acute anterior wall non-ST-segment elevation myocardial infarction (cardiac function class I), high risk of hypertension class 3
(3) Prescription medication:
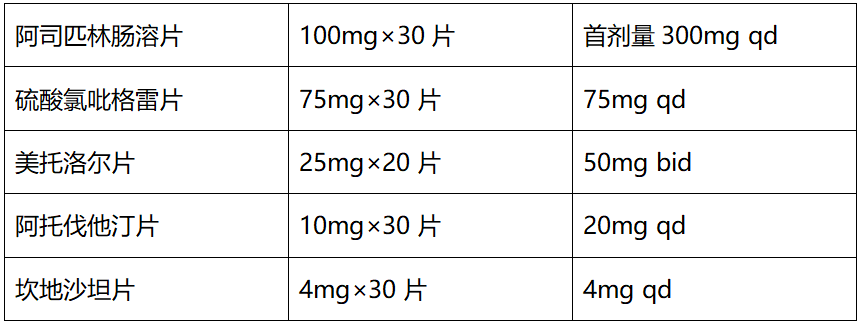
(4) Prescription analysis:
Choose candesartan is unreasonable:
ACEI is the basic drug for hypertension complicated with coronary heart disease and chronic heart failure. According to the “Chinese Expert Consensus on the Application of Angiotensin Converting Enzyme Inhibitors in Cardiovascular Diseases” [9]: the first choice for ST-segment elevation acute myocardial infarction, non-ST-segment elevation acute myocardial infarction and unstable angina pectoris in ACS ACEI drugs; ACEI drugs are also recommended for secondary prevention of coronary heart disease and patients at high risk of cardiovascular disease. ARB drugs are recommended for patients who cannot tolerate ACEI. ARB has no obvious advantage over ACEI in improving the prognosis of patients with coronary heart disease.
Therefore, the patient has no contraindications to ACEI, no symptoms such as dry cough, and ACEI drugs should be the first choice, which is more in line with evidence-based evidence.
References:
[1] Guidelines for Rational Drug Use in Hypertension (Second Edition), Chinese Journal of Medical Frontiers (Electronic Edition), 2017, 7(9):28-123.
[2] Enalapril Maleate Instructions.
[3] Instructions for Telmisartan.
[4] Song Wenxuan, Li De’ai, Practical Cardiovascular Pharmacology, People’s Health Publishing House.
[5] Chinese Guidelines for the Management of Renal Hypertension 2016 (abbreviated version), Chinese Journal of Medicine 2017, 5, 20: 1547-1555.
[6]Expert Suggestions on Clinical Diagnosis and Treatment of Special Types of Hypertension, Chinese General Medicine, 2020, 4, 10: 1202-1228.
[7] Guidelines for Rational Drug Use in Heart Failure (2nd Edition), 2019, 7(11): 1-78.
[8] Chinese Guidelines for the Prevention and Treatment of Hypertension Revision 2018, Prevention and Treatment of Cardiovascular and Cerebrovascular Diseases, 2019, 1(19): 1-44.
[9] “Chinese Expert Consensus on the Application of Angiotensin Converting Enzyme Inhibitors in Cardiovascular Diseases”.
This article was first published: Cardiovascular Channel of the Medical Community
The author of this article: Jin Xiaoqin
Review of this article: Jiehui Zhao
Editor in charge: Yuan Xueqing, Zhang Li
Copyright Notice
This article is original, please contact authorization for reprinting
-End-
The medical community strives for the accuracy and reliability of its published content when it is reviewed and approved, but does not make any guarantees about the timeliness of the published content, and the accuracy and completeness of the cited materials (if any), etc. Any commitments and guarantees, and do not assume any responsibility due to the outdated content, the possible inaccuracy or incompleteness of the cited information. Relevant parties are requested to check separately when adopting or using it as a basis for decision-making.