Recently, Xiang Canhong, chief physician of the Department of Hepatobiliary and Pancreatic Surgery, Beijing Tsinghua Chang Gung Hospital affiliated to Tsinghua University, and Xu Guangxun, deputy chief physician, performed an operation on a patient with hilar cholangiocarcinoma and extensive invasion of the liver. After nearly 17 hours, the patient was resected. Nearly 60% of the diseased livers, including the left third area of the liver, were reconstructed by “bypassing” the hepatic artery, which solved the problem of blood supply to the remaining liver.
Hilar cholangiocarcinoma is a common malignant tumor of the biliary system. Because of its special location, invasive growth and close relationship with the hilar blood vessels, it often causes great difficulty in surgical resection. .
In the famous Japanese liver research center, Nagoya University, 50% of the patients who died were left tertiary resection. At the time of onset, patients may have symptoms such as loss of appetite, indigestion, abdominal pain, skin pruritus, weight loss, and bile duct infection.
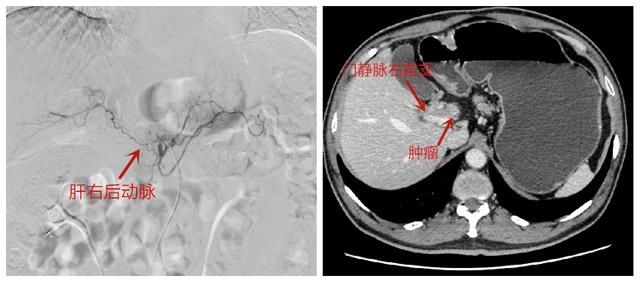
Patient preoperative right posterior hepatic artery (left) and portal vein (right) images
Patient From Henan, he was diagnosed with hilar cholangiocarcinoma due to physical examination. The operation was difficult and risky. After being recommended by the local hospital, he came to Xiang Canhong’s clinic of Tsinghua Chang Gung Hospital in Beijing to seek further treatment.
After perfecting the whole abdominal contrast-enhanced CT examination, it was found that the tumor had invaded the left lateral lobe, left inner lobe, right anterior lobe, portal vein and right posterior hepatic artery. The right posterior hepatic artery, which has been invaded by 5 cm by the tumor, also needs to be resected, and such patients are often considered to be extremely difficult to undergo radical surgery.” Xiang Canhong said that the right posterior hepatic artery is responsible for supplying blood to the right posterior lobe of the liver. The key role, if the whole is removed, may lead to liver abscess, necrosis and even liver failure due to insufficient blood flow.
“For hepatobiliary and pancreatic surgeons, although the left third region resection of hilar cholangiocarcinoma is a difficult hurdle for hepatectomy, they must be brave enough to undertake and challenge.” For this reason, Xiang Canhong After communicating with Xu Guangxun, the deputy chief physician with rich experience in liver transplantation and vascular anastomosis, he finally formulated a surgical plan: reconstruction of the right posterior hepatic artery through “bypass” surgery.
The difficulty of surgery is far from that. “In order to remove the tumor, the operation is expected to remove nearly 60% of the liver, and it is necessary to ensure that the remaining liver has sufficient compensatory function.” Xiang Canhong said. After preoperative examinations such as hepatic arteriography to clarify the liver image and blood supply, Xiang Canhong first performed embolization of the proper hepatic artery to reduce the blood flow of the proper hepatic artery, widen the channel of the right posterior hepatic artery, and increase the blood flow; The right anterior branch of the portal vein is embolized to reduce the blood flow of the liver that has been invaded by the tumor, so that the volume of the liver will shrink and become smaller. .

Xiang Canhong (second from right) undergoing surgery
Perfecting the surgical plan and pre-operative preparations After that, the operation was officially launched. Xiang Canhong was the chief surgeon and Xu Guangxun cooperated to perform “radical resection of hilar cholangiocarcinoma” for the patient.
After the laparotomy, Xiang Canhong and the attending physician Wang Liang carefully dissociated and dissected the liver blood vessels, and protected the right posterior artery of the liver. Then they found the right gastroepiploic artery and took 5 cm of it as a spare. Ligation is then performed as a spare blood vessel for “bypass”.

Xu Guangxun performed surgery
After resection of the middle right posterior hepatic artery invaded by the tumor, transplant The team’s chief physician, Xu Guangxun, Ye Shengji took the stage and used the prepared right gastroepiploic artery to anastomosed with the right posterior hepatic artery on the preserved side, and finally completed the “bypass” reconstruction of the arterial blood vessel.
After the arterial blood supply to the liver was restored, Xiang Canhong came to power again to standardize the enlarged left third region tumor resection and dissection of the surrounding lymph nodes.
Finally, Xiang Canhong excised the part of the portal vein invaded by the tumor and performed anastomosis reconstruction. In order to ensure the patency of the bile duct, Xiang Canhong reshaped the remaining two bile ducts of the sixth and seventh segments of the liver into one bile duct. Open the opening and carefully perform cholangiojejunostomy. By 2 am the next day, the operation was successfully completed. When he was discharged from the hospital, the patient wrote excitedly in the thank you letter: “The well-deserved guardian of life!”
Source: Beijing Tsinghua Chang Gung Memorial Hospital affiliated to Tsinghua University