For medical professionals only
What should I do with the extra “lungs”?
Writing | Preserved Egg and Lean Meat Week
Source | “Medical Community”Pediatrics Channel
The human lung is divided into two sides, the left oblique fissure is divided into 2 lobes, and the right is divided into 3 lobes, which are responsible for breathing. If “one lung” is longer, will people’s breathing ability be stronger?
Recently, the Children’s Hospital Affiliated to Zhejiang University School of Medicine admitted such a child: According to the description of the child’s mother, the child was suspected of having “isolated lung” during the obstetric examination. After birth, her physical fitness is good, but she is more likely to catch a cold than her peers, so she has not taken follow-up treatment. When the child was 6 years old, in order not to affect the child’s future life, the mother brought the child to the hospital for treatment.
After examination, the child was diagnosed with extralobar pulmonary sequestration and underwent surgical resection.

Pulmonary sequestration is a rare congenital malformation of broncho-pulmonary development, accounting for 0.15% to 6.45% of all lung malformations[1], depending on whether there is an intact pleura on the surface of the abnormal lung tissue Separated from normal lung tissue, it is divided into intralobar type and extralobar type. The extra lung is actually a cystic lesion, which not only does not enhance the breathing ability, but does not have any breathing function.
In order to understand the main points of diagnosis and treatment of pulmonary sequestration, “Medical Pediatrics Channel” talked to Tan Zheng, Deputy Director of Thoracic Surgery, Children’s Hospital Affiliated to Zhejiang University School of Medicine, let’s talk about Get up and see, what should I do with this extra “lung”?
1
The symptoms of this disease are not obvious, and it is easy to confuse the eyes
Should the symptoms of pulmonary sequestration be based on pulmonary symptoms? Deputy Director Tan Zheng introduced that the clinical symptoms of intralobar and extralobar pulmonary sequestration are very different due to the different location of the isolated lung [2].
YeAppearance – “I’m asymptomatic and you don’t always recognize me.”
Extralobar pulmonary sequestration often presents as asymptomatic or mild symptoms because the isolated lung is separated from the normal lung and does not communicate with the bronchi. In addition, extralobar cystic lesions are mostly located between the left lower lobe and the diaphragm, or below the diaphragm or in the mediastinum, and are easily misdiagnosed as posterior mediastinal tumors and diaphragmatic tumors.
Once there are significant symptoms of this type, it is mostly caused by torsion of the blood vessels. The lobar appearance provides the anatomical basis for torsion. If the blood vessel is torsion, it can lead to isolated pulmonary ischemia and infarction [3]. The clinical manifestations are mainly abdominal pain, and a few patients have dyspnea, chest pain, chest tightness, and vomiting.
Intralobular – “I have symptoms, but you can easily mistake me for someone else.”
The cystic lesions of intralobar pulmonary sequestration can directly or partially communicate with the bronchi, which makes the isolated lung susceptible to repeated infections. Clinical symptoms are common, but nonspecific, mostly fever, Cough, chest pain, expectoration of purulent sputum or even purulent sputum with blood and recurrent pneumonia, etc., are easily misdiagnosed as lung tumors, lung abscesses, and bronchiectasis.
Professor Tan Zheng mentioned: “Intralobar type, because the isolated lung is connected to the normal lung, has abundant arterial blood supply, the probability of infection is very high, and it also shows some bleeding symptoms. We have encountered A 10-year-old child presented with repeated hemoptysis, and it was found to be an isolated lung of the intralobar type.”
Pulmonary sequestration lacks specific manifestations in clinical manifestations, physical examination and routine laboratory tests, which brings great challenges to clinical diagnosis. This reminds clinicians to exclude pulmonary cysts, bronchiectasis, pneumonia, tuberculosis, lung tumors, diaphragmatic hernia, etc. After illness, pulmonary sequestration should be highly considered and further diagnosis should be made.
2
If you can’t tell the difference, how can you use the auxiliary inspection to refine your eyes?
According to clinical observations and literature reports, the abnormal blood supply arteries of the disease are more common in the lower thoracic aorta, followed by the abdominal aorta and intercostal arteries [4]. Therefore, the detection of abnormal blood supply is the key point in diagnosing the disease.
Chest X-ray: Used primarily for initial screening. Abnormal lung shadows and pulmonary inflammatory manifestations can be found, but they are not specific and are not the first choice. To distinguish the type of pulmonary sequestration, chest CT should be supplemented.
CT of the chest: Contrast-enhanced helical CT scan of the chest or CT 3D reconstruction angiography may be the first choice. Imaging manifestations are solid mass shadow, cystic, patchy shadow, cystic-solid shadow and other two or more kinds of manifestations [5]. In addition, CT can also determine the location, size, number of abnormal blood supply arteries and the relationship with the aorta of the isolated lung.
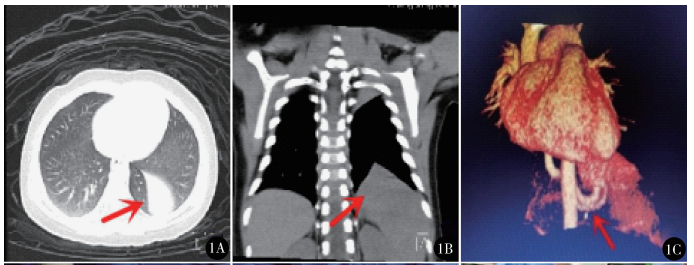
Preoperative CT findings of extralobar pulmonary sequestration: A. “teardrop-like” lesions in the left thoracic cavity; B. “crater-like” signs of extralobar isolated lungs, lesions The border is clear; C. Isolate the abnormal blood supply artery of the lung lesion originating from the abdominal aorta[3]
Intralobar isolated lung enhanced CT findings: A. Enhanced lesions in the right lower lobe; B. Aortic branch blood supply, blood vessel diameter 3. 4 mm; C. Aortic revascularization, Abnormal branches from the aorta can be seen[6]
Magnetic Resonance (MRI): Can detect a well-circumscribed mass within the chest and its internal structure, and can also show the origin, course, and veins of abnormal arteries Backflow situation.
Ultrasonography: If pulmonary sequestration occurs during the fetal period, the fetal lung tissue will not develop properly, pleural effusion, mediastinal displacement, etc. There is a higher chance of intrauterine death. Therefore, early diagnosis has important clinical significance for the disease. Ultrasonography has become the first choice for the diagnosis of fetal pulmonary sequestration due to its advantages of simple operation, strong reproducibility, and no radiation damage.
When the fetus has pulmonary sequestration, a round or oval hyperechoic mass or a slightly hyperechoic mass with clear boundary and regular shape can be seen on ultrasound, and cystic areas of different sizes can be seen by tracing the blood vessels. If there is infection, scattered small light spot reflections can be seen [7].
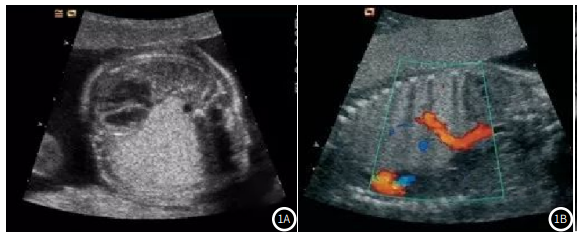
Ultrasonographic images of fetal pulmonary sequestration at 16 weeks of gestation[7]
Deputy Director Tan Zheng reminded that If the fetus is suspected of having pulmonary sequestration during the obstetric examination, it can be transferred to the Children’s Hospital for diagnosis after the fetus is born.
3
Excessive “lung”, surgical resection as soon as possible
For children who have been diagnosed with pulmonary infection, there is still the possibility of repeated secondary infection after conservative treatment, and a small number may also become cancerous. Therefore, pulmonary sequestration should be considered once diagnosed. Surgical excision treatment. Compared with traditional thoracotomy, thoracoscopy has the advantages of less trauma, less postoperative pain, and faster recovery, and has become the mainstream treatment method.
Deputy Director Tan Zheng mentioned that the difficulty of surgical resection is different for extralobar and intralobar type, and intralobar type is mainly lobectomy , or the resection of a lung segment, which is basically similar to the surgical method of adult lung cancer. At the same time, attention should be paid to the treatment of blood vessels, which is one more step than normal lobectomy and segmentectomy, that is, to deal with the blood vessels of the systemic circulation. Due to the separate vascular supply, the extralobular type is relatively simple to handle, including the treatment of systemic blood vessels and returning veins. Some extralobar isolation lungs will grow in the diaphragm or even in the abdominal cavity. In this case, the isolation lung needs to be found first.
“We generally recommend children under 4 years of age to undergo resection as soon as possible. At this time, the child’s lungs still have regenerative function, and the operation will not affect the child’s normal lungs. The current technology allows for day surgery for lung tissue lesions, that is, 24-hour admission and discharge. The trauma during the entire operation is very small, helping the child recover as soon as possible after the operation and grow up as healthy as a normal child.” Deputy Director Tan Zheng Say.
Professional Profile

Tan Zheng
Deputy Chief Physician
Deputy Director of Pediatric Thoracic Surgery and Deputy Director of Surgical Endoscopy Center, Children’s Hospital Affiliated to Zhejiang University School of Medicine
Member of the Thoracic Surgery Group of the Pediatric Surgery Branch of the Chinese Medical Association
China Maternal and Child Health Association Maternal and Child Minimally Invasive Professional Committee Standing Committee Member of Pediatric Extrathoracic Minimally Invasive Group
National Member of the Maternal and Child Minimally Invasive Professional Committee of the China Maternal and Child Health Association
Member of the Pediatric Oncology Committee of Zhejiang Anti-Cancer Association
Member of the Thoracic Surgeons Branch of Zhejiang Medical Association
Member of Pediatric Surgery Branch of Zhejiang Medical Association
Youth Committee of Pediatric Surgery Branch of Zhejiang Medical Association
Undertake and participate in 10 provincial and ministerial projects. Participated in the compilation of 10 books and textbooks on pediatric thoracic surgery, and published more than 20 academic papers, 2 of which were included in SCI. The first in China to obtain the fourth-generation Da Vinci robot pediatric surgery chief surgeon qualification certificate. The pediatric surgeon who achieved the milestone of 100 robotic surgeries in the shortest time in China. The first international pediatric thoracic surgeon to achieve the 100-case robotic milestone.
References:
[1]Chen Gang, Chen Zhanggen, Jia Bing, Li. 22 cases of pulmonary sequestration in childrenAnalysis[J].Fudan Journal (Medical Edition),2006,33(5):683-685.
[2] Yang Jingjing, Li Yumei. Clinical analysis of 16 cases of pulmonary sequestration [J]. China Health Nutrition, 2021,31(33):29-30.
[3] Li Xiao, Cai Chun, Sun Yuling, Du Mengwei, Zhang Gang, Yan Xiangang, Zhou Xiaotong, Yu Gang. Treatment of infantile extralobar sequestration by single-port thoracoscopic technique[J] .Chinese Journal of Minimally Invasive Surgery, 2021,21(10):923-926.
[4] Zhu Yufeng, Bai Yuan, Li Hu, Xue Wang, Qin Yongwen. Clinical research on imaging diagnosis and interventional therapy of pulmonary sequestration[J].South China Journal of Defense Medicine,2018,32 (3):161-164,172..
[5]Tashtoush B, Memarpour R, Gonzalez J, et al. Pulmonary sequestration:
A 29 patient case series and review[J]. Journal of Clinical & Diagnostic Research Jcdr, 2015, 9(12): AC05.
[6]Su Yun, Wu Yurui, Zhang Xiaolun, Liu Jing, Li Zexi. Laparoscopic treatment of 65 cases of children with pulmonary sequestration [J]. Chinese Journal of Minimally Invasive Surgery, 2021, 21(10) :899-903.
[7] Xiong Jing, Chen Qian, Chen Huayan, Chen Lin. Analysis of clinical application value of ultrasound and magnetic resonance examination in fetal pulmonary sequestration [J]. Chinese Journal of CT and MRI, 2021 ,19(6):77-78,102.
Source: Medical Pediatrics Channel
Editor in charge: Jun Ling
Proofreading: Zang Hengjia
Plate making: Xue Jiao