*For medical professionals only
Be wary of atypical symptoms of COVID-19.
The recent epidemic has been fierce. Let us review a case of acute pancreatitis caused by the new crown.
Case presentation
Patient, female, 67 years old.
Complaints: Epigastric pain with nausea and vomiting for 1 day.
Comorbidities: History of hypertension, controllable. He denied the history of diabetes and cholelithiasis.
Prior history: Exploratory laparotomy + small bowel resection and anastomosis due to superior mesenteric artery embolism 1 year ago; apixaban was regularly taken postoperatively.
Personal history: Denies smoking and alcoholism; Denies close contact with COVID-19 patients.
Vital signs: Body temperature 37.5℃, heart rate 112 beats/min, blood pressure 158/90mmHg. (Unfortunately, the original report did not describe the abdominal examination results)
Diagnosis and Treatment
In view of the patient’s past medical history, it is necessary to first consider whether there has been an adhesive intestinal obstruction, and secondly, be alert to the recurrence of mesenteric vascular embolism. At the same time, the patient’s symptoms are also related to acute pancreatic Inflammation, acute gastroenteritis and other identification.
Therefore, the patient directly underwent contrast-enhanced CT of the abdomen and pelvis, and it was found that the pancreatic head and body were not significantly enhanced, and extensive peripancreatic fluid accumulation suggested necrotizing pancreatitis possible (Fig. 1 left). Subsequent CTA showed no obvious thrombus, and progression of the disease was found (Fig. 1, right). Ultrasound examination showed no signs of bile duct stones. Laboratory examination found that blood amylase was 1483 U/L, and liver enzymes, bilirubin, and IgG4 were normal. The other indicators are shown in Figure 2.
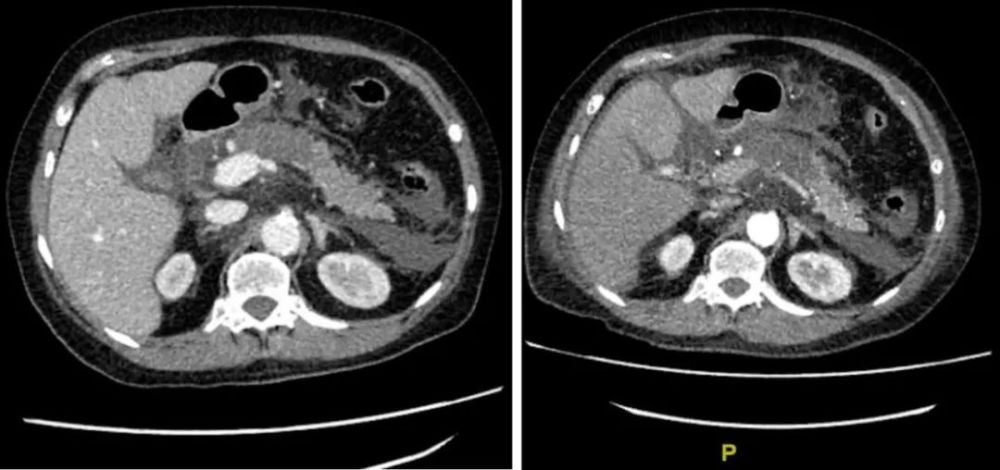
Figure 1: Contrast-enhanced CT of the abdomen on the left, CTA performed on the right afterward
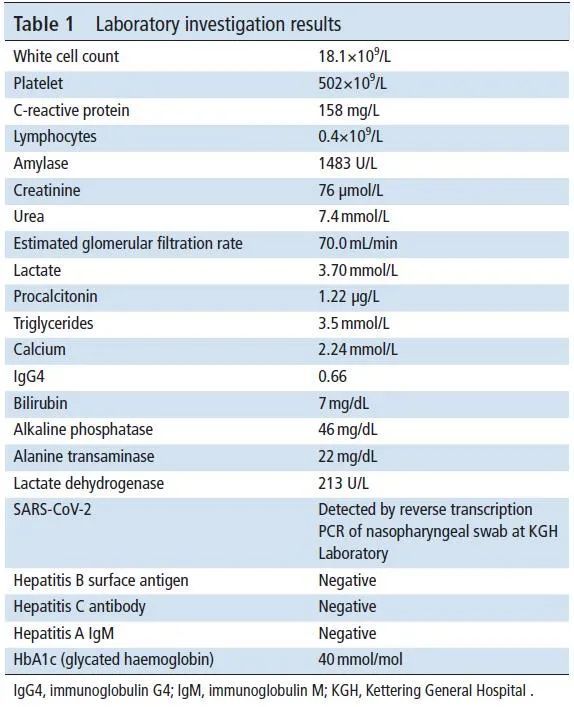
Figure 2: Patient Laboratory Results
Acute pancreatitis is diagnosed by at least two of the following three according to the Revised Atlanta Criteria:
abdominal pain characteristic of pancreatitis;
Elevated serum amylase or lipase to 3 times or more normal levels;
CT, MRI, or abdominal ultrasound findings characteristic of pancreatitis.
There is no doubt that acute pancreatitis was diagnosed in this patient. But what causes acute pancreatitis? The most common biliary factor is currently lacking clear evidence. IgG4 is normal, so autoimmune pancreatitis is not considered for the time being, and the patient has no risk factors such as hyperlipidemia and alcoholism. At this time, the throat swab results of the patient’s admission screening came out – Positive for the new crown!

The patient was quickly isolated. Doctors mainly gave conservative treatment such as fluid resuscitation, but the effect was not obvious. Because the patient’s breathing rate increased (26 breaths/min), the oxygen saturation could only be maintained at 96% under the oxygen flow of 2L/min, so he was sent to the ICU for further monitoring and treatment, and was given successively under the guidance of clinical microbiologists. Antibiotics such as meropenem, metronidazole, and clindamycin were used.
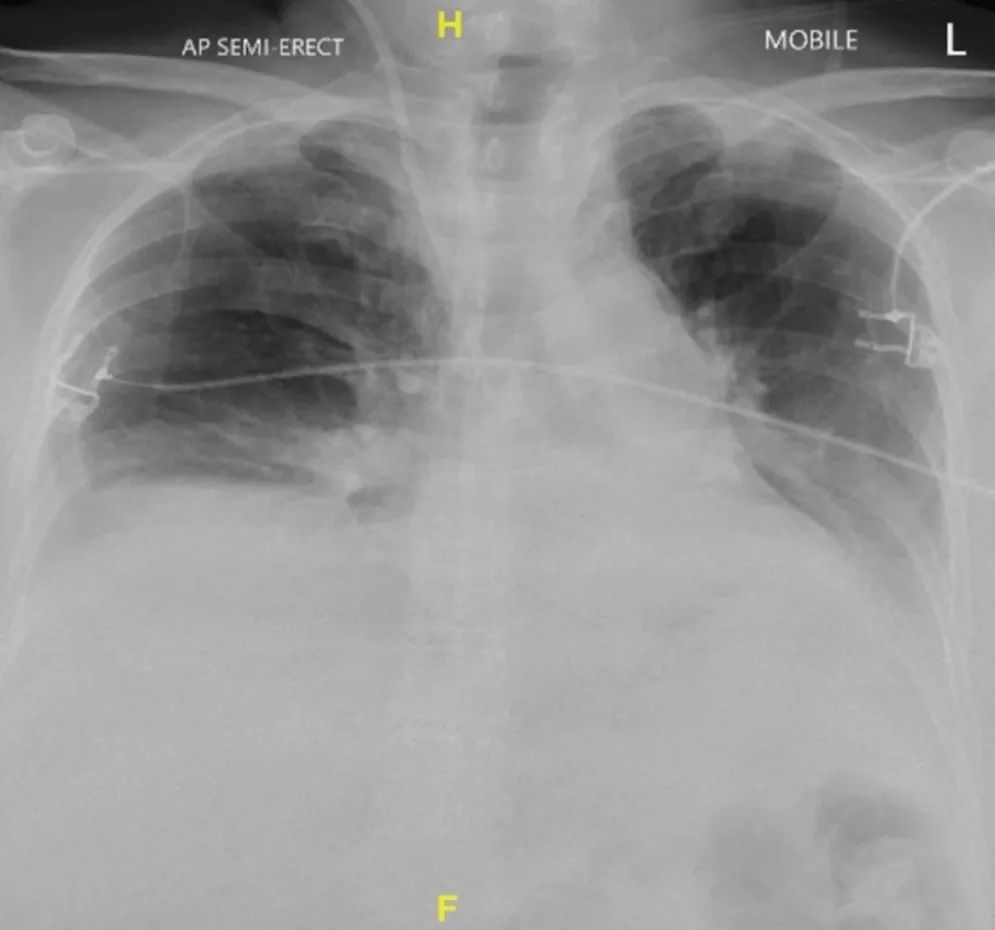
Figure 3: Chest X-ray showed two atelectasis after transfer to ICU
It is worth mentioning that no antiviral, anti-inflammatory or other experimental drugs for COVID-19 were used during ICU treatment, nor was mechanical ventilation or positive Inotropic drugs and other supportive treatment.
The patient returned to the general ward after 10 days of improvement and is currently undergoing rehabilitation physiotherapy.
Experience Summary
Acute pancreatitis has a variety of causes, the most common being biliary and alcoholism, although 10% to 20% of cases have no clear cause. Several pathogens, including viruses, bacteria, and parasites, have also been shown to infect the pancreas. According to literature reports, common viruses that can cause pancreatitis include mumps virus, Coxsackie B virus and hepatitis A virus. Severe pancreatitis caused by coronavirus has been found in pigeons, but no similar reports have been reported in humans.
A study of 52 patients with COVID-19 found that blood amylase or lipase abnormalities were found in 17% of cases, suggesting that these patients may have pancreatic damage. However, to look at this study dialectically, after all, the pancreas is not the only source of amylase production, and gastroenteritis may also cause increased pancreatic enzymes. In addition, studies have confirmed that 18% of new crown patients have gastrointestinal symptoms, so it cannot be directly equated with pancreatitis.
During the 2003 SARS outbreak, some studies examined the cadavers of SARS patients using immunohistochemistry and in situ hybridization, and found SARS virus antigens in pancreatic tissue and RNA presence, confirming that SARS virus can infect the pancreas. The gene sequence similarity between the new coronavirus and SARS virus is as high as 79.6%, and the expression of the new coronavirus receptor ACE2 in pancreatic tissue is even higher than that in lung tissue. It is reasonable to think that the new coronavirus can infect the pancreas. Although the exact pathogenesis of pancreatitis is not known, it is tended to be considered to be cytopathic caused directly by local replication of the virus.
The most serious consequence of COVID-19 is a cytokine storm caused by a dysregulated systemic inflammatory response. Acute severe pancreatitis can also cause systemic inflammatory response syndrome and even multiple organ dysfunction. A variety of inflammatory factors, such as tumor necrosis factor-α, interleukins IL-6 and IL-10, all play a key role in the course of acute pancreatitis and new coronary pneumonia.
Therefore, if acute pancreatitis and COVID-19 coexist, this process may be accelerated. For clinicians, this is quite difficult to deal with. If secondary infection develops from acute pancreatitis, interventions such as necrotic material removal and drainage may be required, posing a great risk of exposure to medical staff involved in the operation.
In short, this case reminds us to pay close attention to the possibility of pancreatitis caused by the new coronavirus during the epidemic, and also to pay attention to personal protection.
Case source:
Kumaran NK, Karmakar BK, Taylor OM.Coronavirus disease-19 (COVID-19) associated with acute necrotising pancreatitis (ANP).BMJ Case Reports CP2020;13:e237903.
References:
1. Wang F, Wang H, Fan J, et al. Pancreatic injury patterns in patients with coronavirus disease 19 pneumonia. Gastroenterology2020;159:367C70.
2. Ding Y, He L, Zhang Q, et al. Organdistribution of severe acute respiratory syndrome (SARS) associated coronavirus(SARS-CoV) in SARS patients: implications for pathogenesis and virustransmission pathways . J Pathol 2004;203:622C30.
3. Liu F, Long X, Zhang B, et al. Ace2 expressionin pancreas may cause pancreatic damage after SARS-CoV-2 infection. ClinGastroenterol Hepatol 2020;18:2128C30.
This article was first published: Medical Surgical Channel
The author of this article: One Poison G
Editor in charge: XU
Copyright Notice