Pleural infection is an infectious disease that occurs in the pleura and pleural cavity, and its morbidity and mortality are on the rise worldwide. According to statistics, the incidence of patients in the United States has reached 90,000 person-times per year, and the hospitalization rate has nearly doubled from 3.96/100,000 in 1996 to 8.1/100,000 in 2008. The mortality rate within one year can reach more than 20%, and the mortality rate can be as high as more than 30% for elderly patients over 65 years old and immunosuppressed patients.
I. Questions about pleural infection
1. Category
Pleural infection is classified into three categories according to the nature of the effusion, simple parapneumonic effusion, complex parapneumonic effusion and empyema. Simple parapneumonic effusion usually requires only antibiotic therapy. In addition to the use of antibiotics, complicated parapneumonic effusions require minimally invasive (thoracentesis, thoracic catheterization) or invasive (eg, surgery) interventions. Empyema refers to the late stage of parapneumonic effusion, when pathogenic bacteria invade the pleural cavity and produce purulent exudate accumulation, which must be continuously drained from the pleural cavity.
Pleural infection is classified into community-acquired pleural infection and hospital-acquired pleural infection according to the site of infection. Community-acquired pleural cavity infection refers to pleural cavity infection acquired outside the hospital, including pleural cavity infection with definite incubation period pathogen infection and pleural cavity infection onset within the incubation period after admission. Hospital-acquired pleural infection refers to pleural infection that develops after 48 hours of hospitalization, or as a result of invasive thoracic surgery and other iatrogenic causes. The fatality rate of hospital-acquired pleural cavity infection is much higher than that of community-acquired pleural cavity infection, but the incidence rate is lower than that of community-acquired pleural cavity infection. Hospital-acquired pleural infection is usually secondary to hospital-acquired pneumonia, trauma, or surgery. Most of the current research on pleural cavity infection is mostly community-acquired pleural cavity infection as the research object. The consequences of hospital-acquired pleural cavity infection are more serious and the mortality rate is higher, and clinical attention needs to be further increased.
2. Pathways for pathogenic bacteria to enter the pleural cavity
Pathogens enter the pleural cavity through the following aspects:
Translocation of bacteria into the pleural space through adjacent lung parenchyma
Visceral pleural injury or pleural fistula formation
Hematogenous spread
Parietal visceral pleural penetrating injury
Transmediastinum transmission
Transdiaphragmatic spread
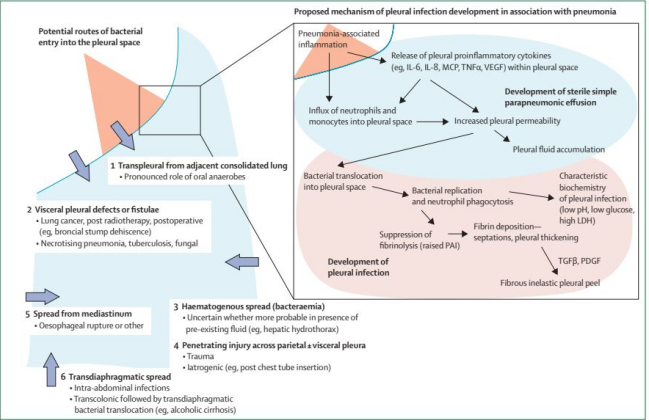
Figure 1
3. Development of pleural effusion and pleural infection
The development of pleural effusion and pleural infection includes three stages: exudative stage, fibro-purulent stage, and organizing stage.
4. Diagnostic techniques for pleural infection
Diagnostic techniques for pleural infection include the following:
•Histopathology: Gold standard, but limited in application because it is an invasive procedure.
●Microbial examination and culture: It takes a long time, and the positive rate is only 30%-40%.
●16sRNA technology: It is highly specific and conservative, and the detection can be completed in 2 hours.
●Metagenetic next-generation sequencing: comprehensive coverage of pathogens, but cannot distinguish infection, colonization or contamination.
5. Distribution of pathogenic sources of pleural infection
The distribution of pathogenic sources of pleural cavity infection is affected by many factors, including pathogenic bacteria invasion route (lung parenchyma, hematogenous, mediastinal, etc.), infection environment (hospital, community, etc.) ), age and immune function status, the composition of oral pathogens (aspiration factor), and the location of the patient.
There are many related studies at home and abroad on the distribution of pathogens of pleural cavity infection. We can look at some international studies on the distribution of pathogens related to pleural infection (Figure 2), such as this study conducted in Australia in 2014, which studied the distribution of pathogens in 713 patients.
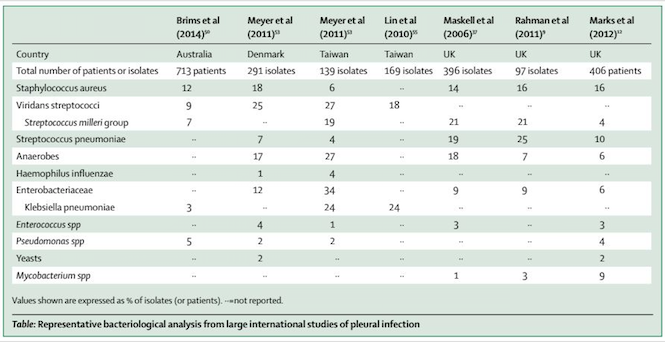
Figure 2 Lancet Respir Med 2015; 3: 563C77
In China, the pathogenic bacteria of pleural cavity infection were analyzed through relevant research. A survey by the National Bacterial Resistance Detection Network showed that a total of 75,375 bacterial strains were isolated from pleural effusion specimens reported from 2014 to 2019. The pathogens were classified as follows: Escherichia coli (10.30%), Staphylococcus epidermidis (8.13%, 2015 data not listed separately), Staphylococcus aureus (8.11%), Klebsiella pneumoniaebacteria (7.51%), Acinetobacter baumannii (5.89%), Pseudomonas aeruginosa (5.86%), Enterococcus faecium (5.24%), Enterococcus faecalis (3.46%), etc. (as shown in Figure 3).
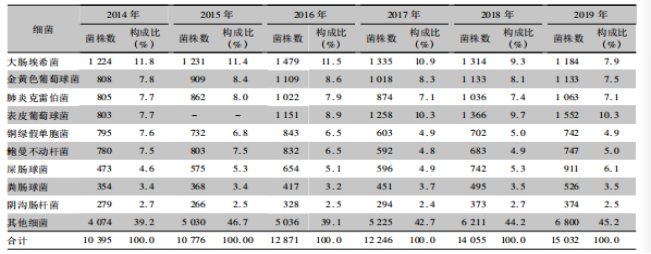
Figure 3
6. Comparison between hospital-acquired pleural infection and community-acquired pleural infection
The pathogens of hospital-acquired pleural cavity infection are different from those of community-acquired pleural cavity infection. There are more negative bacteria in hospital-acquired pleural cavity and relatively few positive bacteria. Community-acquired pleural infection pathogens (such as Streptococcus, Staphylococcus aureus, etc.) positive bacteria accounted for a higher proportion. You can see related studies (Figure 4, Figure 5), because the pathogens of hospital-acquired pleural cavity infection and community-acquired pleural cavity infection are different, so we must first determine whether it is a community infection or a nosocomial infection, so that The choice of antibiotics for our initial treatment.
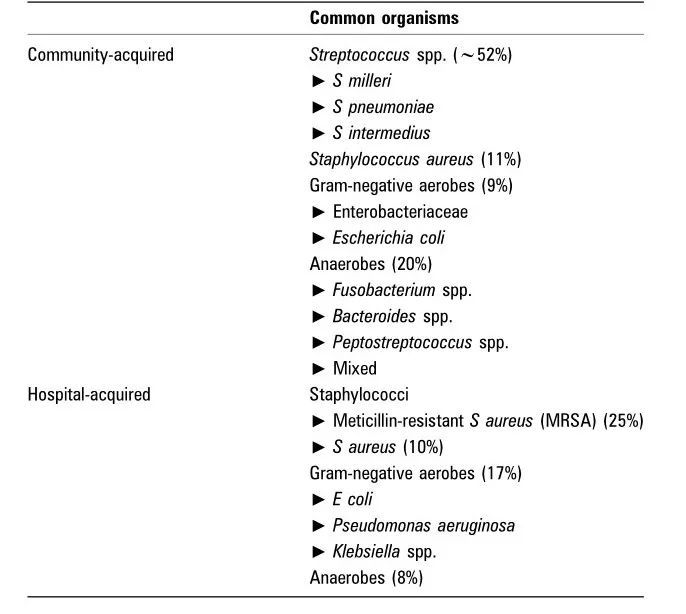
Figure 4: Thorax 2010;65(Suppl 2):ii41-53
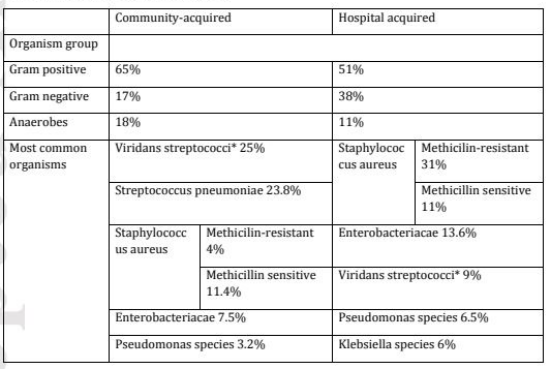
Figure 5: Clin Respir J. 2018 Aug;12(8):2309-2320.
7. Treatment of hospital-acquired pleural infection
The treatment of hospital-acquired pleural infection includes the following:
Effective anti-infection
Adequate drainage of pleural effusion
Nutritional support therapy
Intrathoracic drug therapy
Medical thoracoscopy
Surgical treatment
These treatments focus on nutritional support therapy. Nutritional support treatment is very important for hospital-acquired pleural infection, because hospital-acquired pleural infection has severe systemic poisoning symptoms, high energy consumption, and long treatment time. Nutritional support must be paid attention to to improve the general condition. The treatment time for pleural cavity infection may be 2 to 3 months or even half a year. During this period, diet, intravenous hypernutrient support, electrolyte supplementation, maintenance of water and electricity balance, and albumin supplementation should be adjusted according to the primary disease and systemic conditions.
Indications for drainage of the pleural space include the following:
Pleural effusion is purulent
● pH < 7.2 in patients with suspected chest infection
Separate pleural effusion
Non-purulent pleural effusion identified by Gram stain and/or culture
Large nonpurulent pleural effusion
●Unsatisfied with the above conditions, no improvement after reasonable antibiotic treatment
Indications for intrapleural administration are mainly indications for treatment with compatible drugs. That is to say, when the effect of puncture and drainage after pleural effusion separation is not good, intrathoracic administration should be considered. Fibrinolytic agents can disrupt the separation of pleural fluids, but they cannot reduce the viscosity of pleural fluids. Relevant studies have shown that tissue plasminogen (t-PA) combined with DNase can reduce the viscosity of pleural fluid. However, due to the limited number of patients enrolled in this study, patients with thoracic infection of various stages were included in the study, and most of them were combined with various diseases. These factors have had an impact on the results of the study, and the current treatment needs to be further verified by larger studies.
If the intrathoracic separation package is obvious and the puncture effect is not good, some drugs in the thoracic cavity can be considered. When active drainage combined with intrathoracic drug therapy is still ineffective, medical thoracoscopy can be used to mechanically separate the intrathoracic compartment, and adjust the drainage tube to the lowest position of the abscess cavity to facilitate drainage.
Consider surgery when thoracentesis, intrathoracic drug therapy, and medical thoracoscopic release of intrapleural adhesions are still ineffective. The surgical methods were video-assisted thoracoscopic surgery (VATS) and thoracotomy.
8. Risk factors for death in patients with pleural infection
Several studies have reported on risk factors for death in patients with pleural cavity infection, including a 6-year Australian study suggesting that older age, male sex, elevated CRP, surgery and community-acquired pleural Three-month mortality in patients with cavity infection was correlated. and hospital-acquired pleural infectionThe risk factors associated with three-month mortality were advanced age, male sex, immunosuppression, and the combination of multiple pathogens.
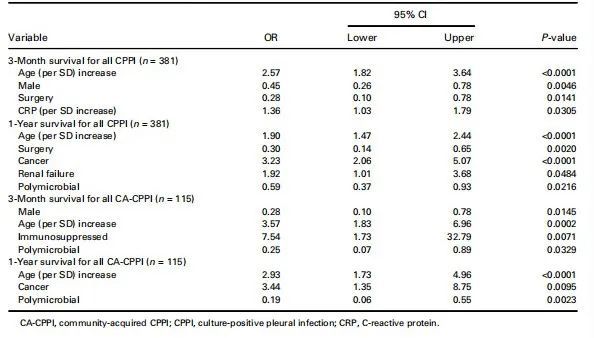
Figure 6: Respirology, 2019, 24(2): 171-178
II. Retrospective analysis of the characteristics and pathogen distribution of adult patients with pleural infection in PLA General Hospital from January 1, 2010 to September 30, 2020
The following introduces a retrospective study of patients with pleural cavity infection in the PLA General Hospital during a 10-year period from January 1, 2010 to September 30, 2020 Hospitalized adult patients with pleural cavity infection. The inclusion criteria are: age ≥ 18 years old with positive microbiological culture of pleural effusion, clinical manifestations of pleural infection such as fever, cough, chills, chest pain, and pleural effusion examination meet one of the following: pleural effusion pH value <7.2, glucose 1000IU/L Antibiotic treatment is required.
1. Selected cases
A total of 832 patients were enrolled in the study, with more men than women, and more patients with hospital-acquired pleural infection than with community-acquired pleural infection.
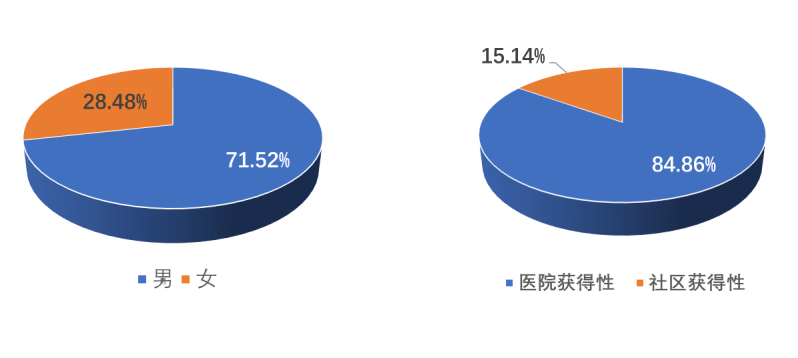
Figure 7
2. Classification of etiology of pleural infection
We classified the etiology of pleural infection, among which pneumonia accounted for 25.96%, malignant pleural effusion with pleural infection accounted for 22.47%, tuberculous pleurisy accounted for 7.9%, surgery/trauma Lead accounted for 22.23%.
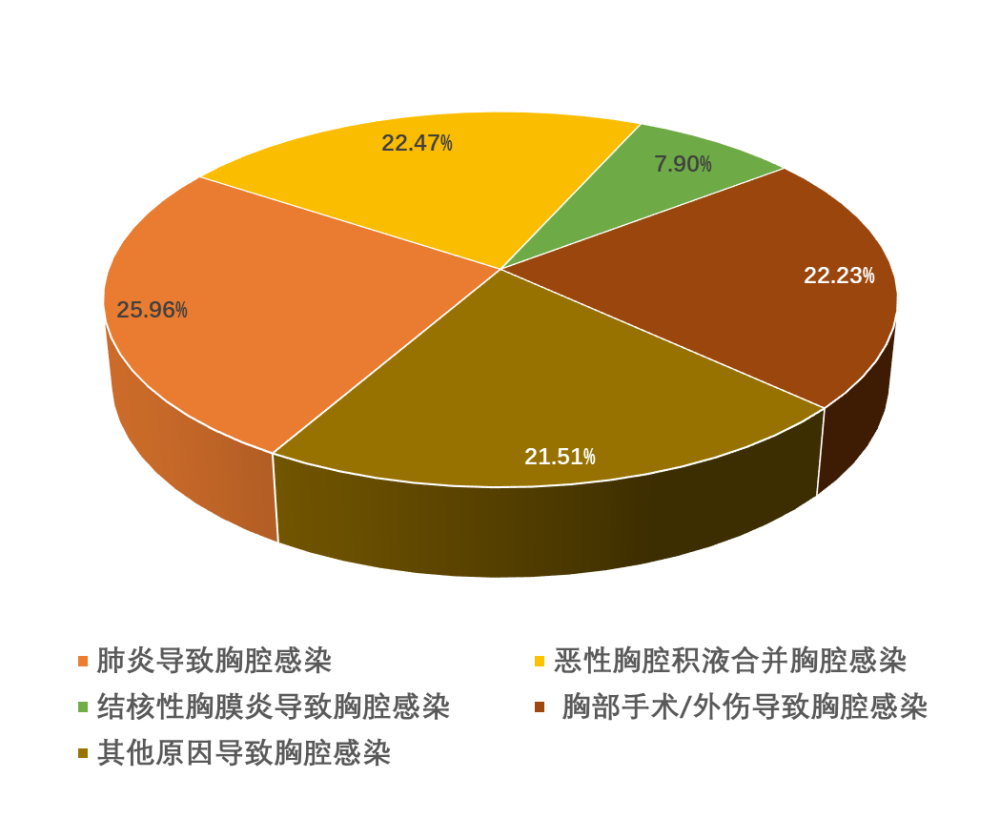
Figure 8
3. Main clinical manifestations
The main clinical manifestations are fever, cough, expectoration, chest pain, dyspnea, but these signs are not specific. Among them, the 30-day treatment outcome was that the cure + improvement rate was 64.07%, and the mortality rate was 13.10%.
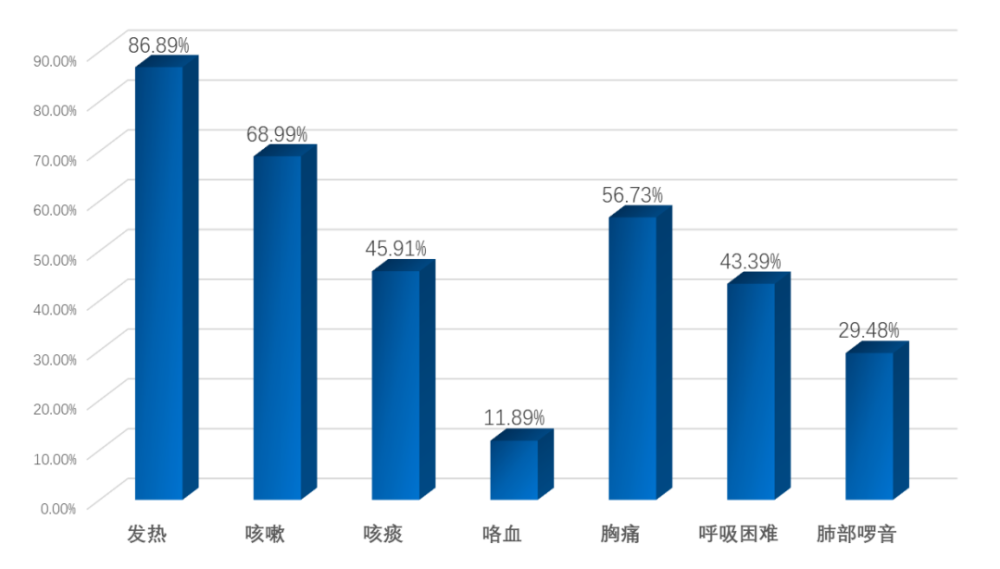
Figure 9
4. Distribution of pathogens
A total of 1066 pathogens were isolated. Common pathogens include coagulase-negative staphylococci, enterococci, Acinetobacter baumannii, and Staphylococcus aureus.
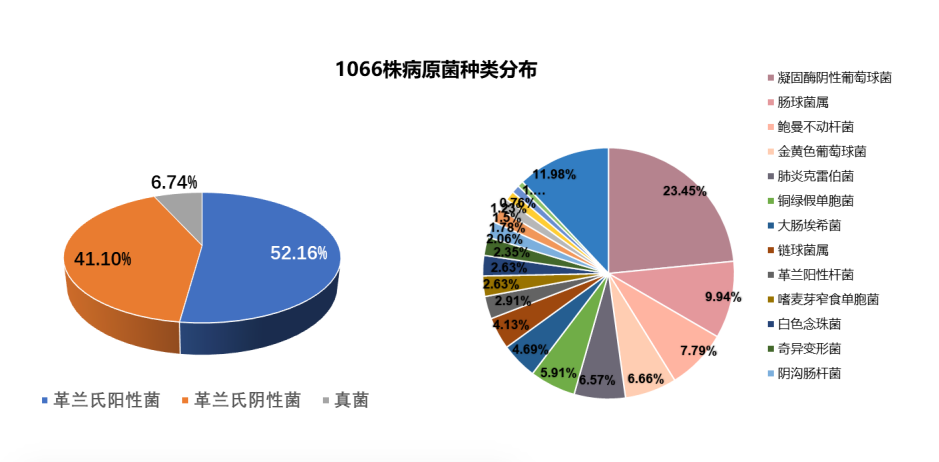
Figure 10
5. Comparison of patients’ basic conditions
Comparing patients with community-acquired pleural cavity infection and hospital-acquired pleural cavity infection, there were 126 cases of community-acquired infection and 706 cases of hospital-acquired infection. A statistically significant difference was the predominance of primary pneumonia causing community-acquired pleural infection. Malignant pleural effusion and thoracic surgery/trauma accounted for a higher proportion of patients with hospital-acquired pleural infection.
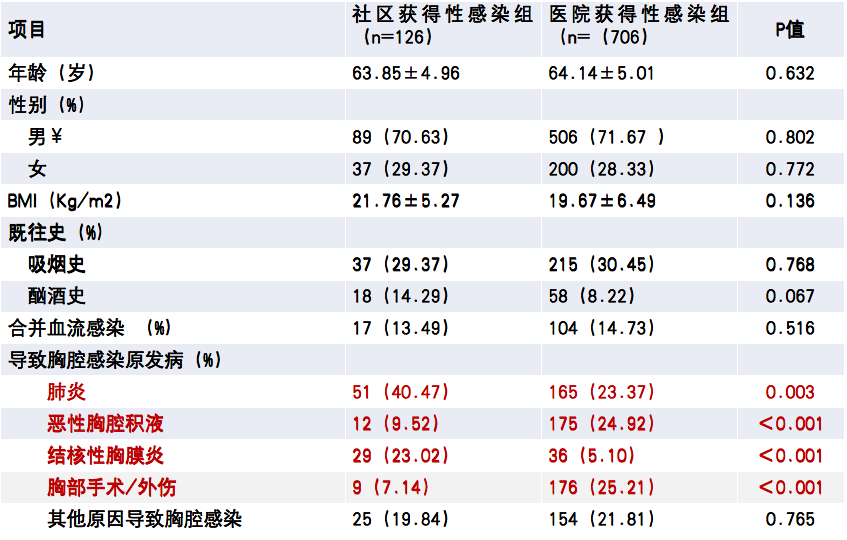
Figure 11
6. Distribution of pathogens
A total of 137 pathogens were isolated from pleural effusion in 126 patients with community-acquired pleural infection. The common pathogens were: Streptococcus (27.01%), coagulase-negative Staphylococcus (14.60%) ), Staphylococcus aureus (12.41%), Enterococcus faecium (6.57%), etc.
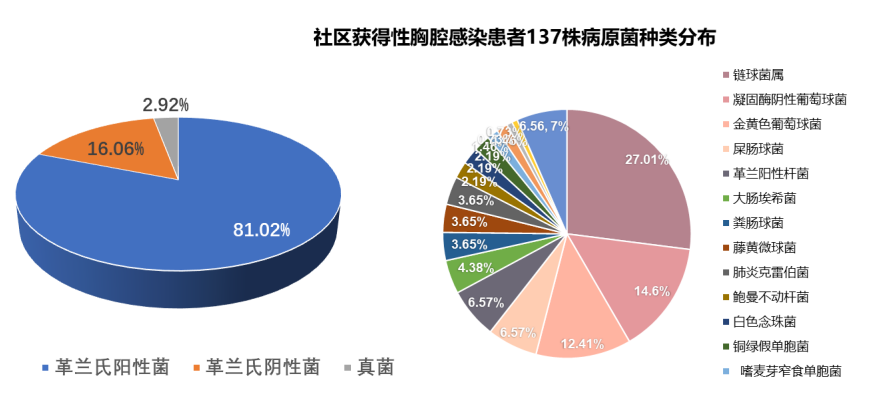
Figure 12
A total of 929 pathogens were isolated from pleural effusion in 706 patients with hospital-acquired pleural infection. The common pathogens were: coagulase-negative staphylococcus (24.76%), Bowman Acinetobacter (8.61%), Enterococcus faecium (7.86%), Klebsiella pneumoniae (6.99%), Pseudomonas aeruginosa (6.46%), Staphylococcus aureus (5.81%), Escherichia coli ( 4.74%) and so on.
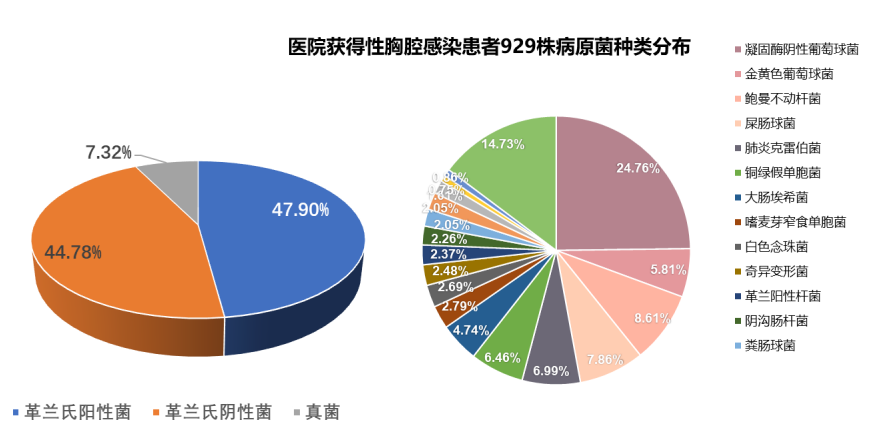
Figure 13
7. Drug susceptibility analysis
We conducted drug susceptibility analysis on these pathogenic bacteria, among which Staphylococcus had the highest resistance rate to penicillin and erythromycin, and had the highest resistance rate to vancomycin, linen Zolamide was 100% sensitive; coagulase-negative staphylococci were higher than Staphylococcus aureus for most of the tested antimicrobials.
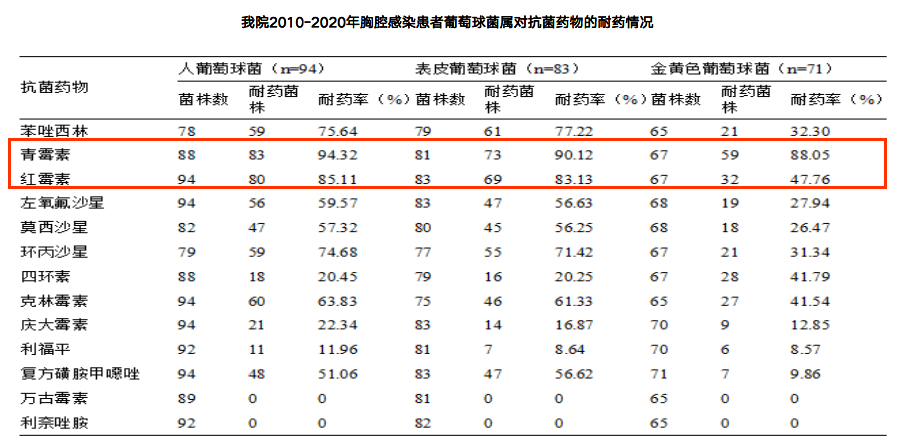
Figure 14
Enterococcus faecium is 100% resistant to oxacillin and clindamycin, and 100% sensitive to tigecycline and linezolid; The resistance rate of Enterococcus faecalis to erythromycin reached 76.19%, and 100% to vancomycin, linezolid and tigecycline; the resistance rate of Enterococcus faecalis to most of the tested antibiotics was higher than Enterococcus faecalis.
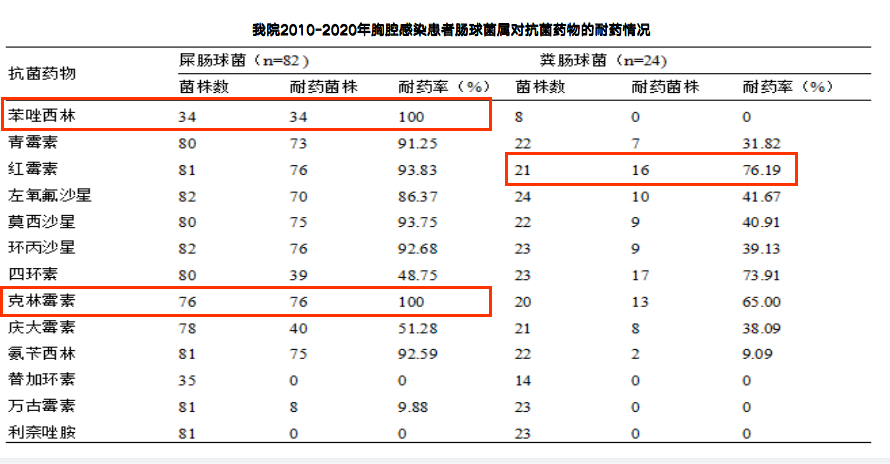
Figure 15
Analysis of drug susceptibility to Gram-negative bacteria: the resistance rate of Acinetobacter baumannii to the tested antibiotics was ≥79.71%; Klebsiella pneumoniae to The resistance rate of amikacin, imipenem, meropenem and ertapenem was less than 20%; the resistance rate of Pseudomonas aeruginosa to imipenem and meropenem was higher than 30%.
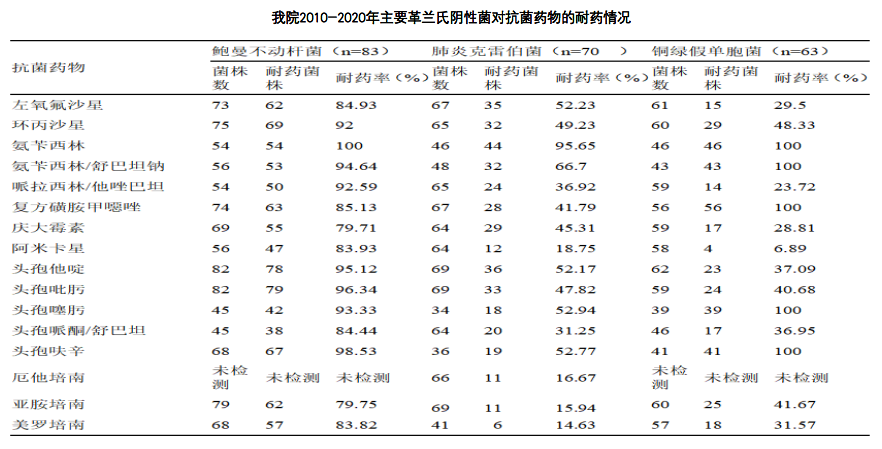
Figure 16
8. Laboratory analysis
In addition, laboratory related examinations found that the level of serum albumin in the hospital-acquired pleural cavity infection group was significantly lower than that in the community-acquired pleural cavity infection group, possibly due to Patients with hospital-acquired pleural cavity infection are often more critically ill, with higher consumption resulting in lower albumin levels.
9. Antibiotic treatment
The results showed that 46.39% of the patients used a combination of 2 antibiotics, 29.81% of the patients used a combination of 3 antibiotics, 13.70% of the patients used a combination of 4 antibiotics, and 10.09% of the patients One antibiotic was used, and the overall case fatality rate was 13.10%. The proportion of the community-acquired thoracic infection group using one antibiotic treatment was significantly higher than that of the hospital-acquired infection group, indicating that the hospital-acquired infection was often more severe. Statistical differences in sexual thoracic infection.

Figure 17
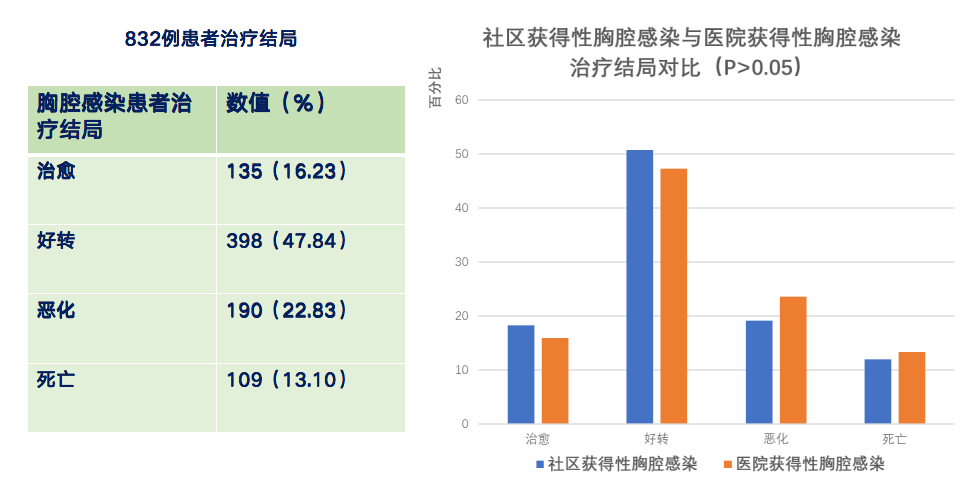
Figure 18
10. Risk factors for death in patients with pleural infection
Analysis of risk factors for death in patients with pleural cavity infection, including demographic characteristics, comorbidities, underlying immunosuppression, invasive procedures, laboratory tests, and treatment methods , found that ICU admission, combined solid tumor, combined renal insufficiency, and decreased serum albumin were independent risk factors for 30-day death in patients with thoracic infection.
11. Summary
The morbidity and mortality of pleural infection are on the rise, and the treatment is full of challenges. The treatment of hospital-acquired pleural infection is difficult, the cycle is long, and the prognosis of patients is poor;
Hospital-acquired and community-acquired pleural cavity infection have many differences in pathogenic distribution and clinical characteristics, and understanding their characteristics can provide reference for anti-infective treatment;
The development of a clinical risk scoring system for hospital-acquired pleural cavity infection and the establishment of predictive models are of great clinical significance and will allow clinicians to develop early treatment strategies for patients based on risk.
Finally, it is expected that domestic prospective, multi-center, large-sample investigations related to pleural infection can provide us with more conclusions to guide our clinical treatment.
Expert introduction

Liang Zhixin
Chief physician, professor and master tutor of Department of Respiratory and Critical Care Medicine of PLA General Hospital; member of Youth Committee of Chinese Medical Respiratory Disease Branch and member of Pleural and Mediastinal Diseases Group; Youth of Chinese Medical Association Internal Medicine Branch Deputy head of the study group; deputy head of the chronic disease prevention working group of the Respiratory Physician Branch of the Chinese Medical Doctor Association; deputy director of the Interventional Minimally Invasive Respiratory Branch of the Chinese Medical Education Association; deputy director of the Youth Committee of the Military Respiratory Medicine Professional Committee.
This article was organized by Sun Yuran, editor of “Respiration World”. Thanks to Professor Liang Zhixin for reviewing and modifying!
End of this article
Typesetting: Jerry
Follow us