Staging a tumor is a consistent and concise way of naming the anatomical extent of tumor invasion. Staging is the cornerstone of diagnosis and treatment. It can predict outcome indicators, facilitate comparisons between different diagnosis and treatment methods, and determine the applicability of clinical trial results to individual patients.
The International Association for the Study of Lung Cancer (IASLC) has leveraged its global multidisciplinary reach to develop a new staging of thoracic malignancies (lung, pleura, thymus, and esophagus) using a sophisticated approach. The 9th edition of the TNM staging of thoracic malignancies is being further refined and will be available in 2024. This article focuses on the specific work of the IASLC in the 9th edition of the TNM staging of lung cancer.
In order to update the 9th edition of the TNM staging for lung cancer, the IASLC has again assembled a large international multicenter database to conduct a multifaceted analysis. The proposed new staging needs to maintain a high degree of consistent discrimination among patients with different clinical backgrounds and diagnosis and treatment patterns.
General process for new staging
Subcommittees of the Staging and Prognostic Factors Committee (SPFC) conduct regular teleconferences and participate in the annual World Lung Cancer Conference organized by the IASLC for communication. Proposals to revise the staging are first developed within the various subcommittees and then presented and discussed at the joint meeting.
After revision and appropriate validation, the proposal will be submitted to the entire SPFC for further revision and formal approval. It is then submitted to the International Union Against Cancer (UICC) and the American Joint Oncology (AJCC), which finalize the 9th edition of the TNM staging for thoracic malignancies.
Data sources for new installments
The 9th edition of the TNM staging database is similar in size to that used for the 7th edition (81,495 cases) and 8th editions (77,156 cases) for lung cancer staging, and includes lung cancer data from at least 25 countries to ensure that It is widely representative.
The database consists of data pre-entered into an Electronic Data Capture (EDC) system from about 50 participating points and “bulk” datasets from various countries and institutions. The data elements of the bulk dataset must be mapped to the data elements of the IASLC database including Cancer Research and Biostatistics (CRAB). Data is primarily sourced from 25 countries in Africa, Asia, Australia, Europe, the Middle East, North and South America.
The IASLC database on Cancer Research and Biostatistics (CRAB) has both advantages and disadvantages. As this is a voluntary database, the SPFC has no ability to control the size, regional distribution or completeness of data elements, other than to encourage participation. The SPFC strongly encourages the use of the EDC system as it leads to more complete data, but is still in the minority at present. Some regions have a disproportionately high proportion of cases (around 70% in Asia/Australia and around 40% in Japan alone), while others have a low proportion of cases (Africa
However, in the new staging version, under-resourced countries and high-staging cases contribute more to the current database than in previous versions, reflecting the IASLC’s direct efforts in these areas.
New staging considerations
OS was the only outcome factor considered at the start of staging. OS metrics are a logical choice when treatment outcomes, access to care, early detection, and data availability are limited. For the 9th edition of the TNM staging, the SPFC still considers OS to be the primary endpoint.
However, for early-stage and indolent tumors, recurrence is considered a more representative measure of the extent of tumor impact. Therefore, the SPFC approach is to first assess clinical relevance, assess factors that may have influenced the observations, and then add statistical assessments to complement the interpretation of the conclusions and increase confidence.
For the calculation of survival time, the survival time was calculated from the date of clinical diagnosis of the tumor and the date of surgical and pathological diagnosis of the tumor, and the Kaplan-Meier method was used for analysis. Cases with missing relevant data were excluded from the analysis. Survival estimates were compared using the likelihood ratio test of Cox proportional hazards regression. Cox regression analysis was performed using SAS version 9.4, adjusting for baseline factors (eg, age, sex, region, cell type).
Attachment: Guidelines for New Stage Development
The existing definitions of T, N, and M should be maintained unless there is compelling evidence to support the change. This will ensure vertical compatibility with previous staging systems wherever possible. (This is less important for stage grouping, as compatibility can be achieved if consistent T, N, and M classes are available).
T, N, and M categories and stages should group tumors of similar clinical significance and distinguish cohorts of different clinical significance.
This should be based on relevant data whenever possible. The key measure is consistent distinction between categories and groups (across different settings, tissue types, global regions, clinical settings [clinical (c) stage, pathological (p) stage, residual tumor (R) status]) to ensure generalizability .
Practical considerations affect clinical relevance (eg, generality, familiarity, ease of use, popularity of features, ease of identifying features, applicability of treatment considerations).
Staging of lung cancer must conform to the general rules for TNM grading of malignant tumors:
The TNM system consists of 3 parts: T is the extent of the primary tumor, N is the extent of regional lymph node involvement, and M is the extent of distant metastases.
Clinical stage (cTNM) includes all available information reflecting the anatomical extent of the tumor before treatment begins. This may involve symptoms, physical examination, imaging, endoscopy, biopsy, and surgical exploration. Therefore, clinical staging and confidence in assessment may vary with patient tumor progression.assessment and development, thereby assessing the extent of the tumor.
Pathologic staging (pTNM) includes all information obtained from surgical resection (or attempted resection) and supplements all available information for clinical staging.
Specific TNM categories can be combined into stage groups.
The definitions of T, N, M categories and stages should be the same for clinical and pathological stages.
The definitions of TNM classes and stages may be adjusted or expanded for clinical or research purposes without changing the basic definitions of TNM classes and stages.
If in doubt as to the correct T, N, or M category to which a case should be assigned, the lower (less advanced) category should be selected.
If an organ has multiple primary tumors, the tumor with the highest T classification should be classified, and the degree or number of tumors should be indicated in parentheses, such as T2(m) or T2(5) . (In lung cancer, this applies to multifocal ground glass adenocarcinoma/squamous adenocarcinoma, but not to isolation of the primary tumor).
Detailed process of new instalment development
1. Planning Phase – Identify potential factors to consider, including:
Disadvantages of version 8 (ambiguity, poor enforceability).
8 Potential heterogeneity within a category or group.
Factors proposed by external analysis (literature).
Factors previously suggested for further analysis (7th or 8th edition).
Factors proposed by stage assessment (imaging, interventions) progression.
Factors proposed for new decision points for therapeutic interventions.
Factors proposed by the SPFC Subcommittee.
2. Implementation Phase – Strategies:
Define the details of the underlying analysis (see related text).
Assessing the 2011-2019 IASLC-CRAB database problem-solving ability (sample size, number of events, prevalence, robustness of internal assessments).
Identify additional data sources that can help analyze specific factors.
Identify the source of external verification.
Select the factors that are feasible for the analysis.
3. Exploratory Analysis:
Collate and evaluate the IASLC-CRAB database (remove errors, evaluate the need for adjustments when combining data of different types/sources, evaluate patterns of missing data).
Generate graphs of relevant outcomes by underlying factors (all cases and across subgroups: such as clinical and pathological settings, relevant T, N, M categories, and relevant treatment modalities).
Assess the acceptability of underlying factors with appropriate clinical relevance and consistent ranking.
Lung cancer tissue type, intra-continental generality assessment across continents.
Identify and analyze additional subsets to address potential confusion and exploration inconsistencies.
Consider supplementary charts for additional outcomes (eg, recurrence, progression) and their interpretation.
4. Confirmatory Analysis and Selection:
Assess differences in underlying factors identified in the exploratory analysis – i.e. assess the statistical significance of differences between adjacent categories, groups (considering clinical relevance and sample size issues – e.g., When sample size limits the power of detection, an ordering that is largely consistent and that trends are not significant may be acceptable).
Assess homogeneity within groups (e.g., confidence intervals for survival parameters, analysis of statistical significance), note that a reasonable demonstration of homogeneity does not preclude the discovery of outliers or additional Parameters that can be used to segment groups.
Factors are selected after a detailed review of the steps to date and discussions within the subcommittee and prior to the SPFC as a whole.
5. Internal and external validation (possibly concurrent with refinement, review and release):
Internal validation of generality, including history, geographic location, method, disease spectrum, follow-up interval, etc.
External validation in appropriate database.
6. Revise, review and publish proposals:
Proposals from each subcommittee are presented and discussed among all members of the association
Draft circulated to all SPFC members for revision and approval
External Journal Review Process
Published in JTO, with open dissemination, open comment ability
7. The International Union Against Cancer (UICC) and the American Joint Oncology (AJCC) accept the final new staging.
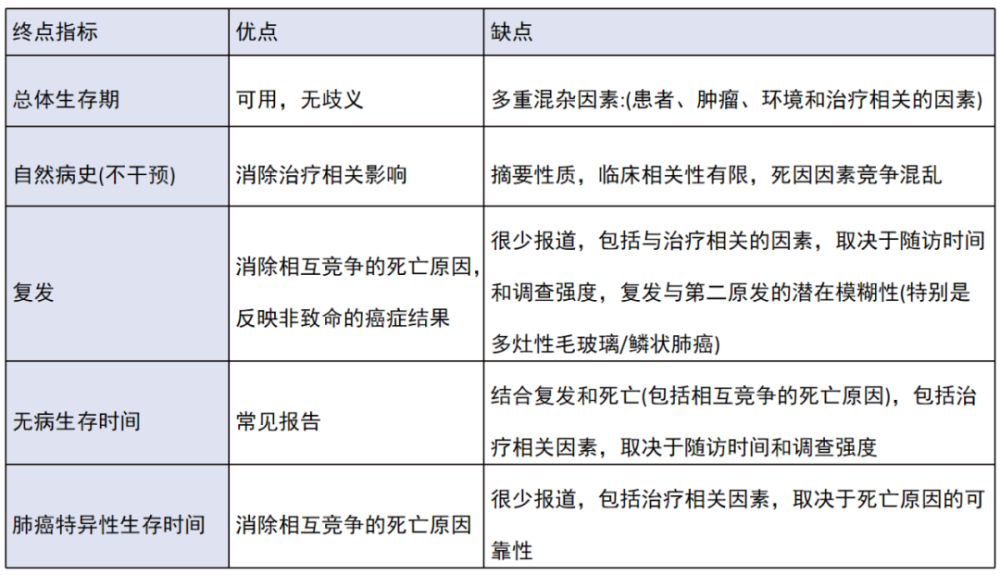
Advantages and disadvantages of using different endpoints for new staging
Image source: courtesy of the author
Planning: GoEun, Mei Zhe
The source of the title map: Zhanku Hailuo PLUS
References
Detterbeck FC, Nishimura KK, Cilento VJ, Giuliani M, Marino M, Osarogiagbon RU, Rami-Porta R, Rusch VW, Asamura H; IASLC Staging and Prognostic Factors Committee and Advisory Boards. The IASLC Lung Cancer Staging Project: Methods and Guiding Principles for the Development of the 9th Edition TNM Classification. J Thorac Oncol. 2022 Mar 9: S1556-0864(22)00107-1. doi: 10.1016/j.jtho.2022.02.008. Epub ahead of print. PMID: 35278692.