*For medical professionals only
Wonderful case sharing~
Pulmonary sarcomatoid carcinoma (PSC) is a rare type of poorly differentiated non-small cell lung cancer (NSCLC) that accounts for less than 1% of all lung cancers. Compared with other NSCLC subtypes, PSCs are more aggressive and have a worse prognosis. According to an analysis by the National Cancer Database (NCDB) and Surveillance, Epidemiology, and Outcomes (SEER) database, the median overall survival (OS) of patients with stage IV PSC is only 3.0 to 5.4 months. Moreover, PSC patients are prone to develop resistance to a variety of chemotherapeutic drugs, and treatment options are very limited.
With the development of genetic testing technology, the genetic map of PSC is gradually becoming clearer. It has been reported that the incidence of MET exon 14 skipping mutations in PSC patients can be as high as 31.8% [1]. MET has emerged as a promising therapeutic target for PSC patients. This article shares with you a case of MET inhibitor treatment of a PSC patient with MET exon 14 skipping mutation [2].
Case profile
A 75-year-old male patient presented in September 2017 with cough, dyspnea, and intermittent chest pain. The patient had a 40-year history of smoking, 40 cigarettes per day.
CT showed that the longest diameter of the lesions in the right lower lobe was 5.6 cm, the right hilar lymph nodes were enlarged, and there were multiple metastases in the right pleura. Biopsy of lung lesions revealed stage IV (T3N1M1) sarcomatoid carcinoma, possibly transformed from adenocarcinoma.
Next-generation sequencing (NGS) of lung biopsy samples revealed MET exon 14 skipping mutation (NM_000245:c.3028+3A>G) with a variant allele frequency (VAF) of 73.9% , which may lead to alternative splicing of the MET protein. In addition, NGS revealed MET amplification, TP53 (V173M) mutation, FBXW7 (G459R) mutation, but no EGFR, KRAS, ALK, and ROS1 gene mutations were detected.
Patient refused chemotherapy and enrolled in a phase II clinical trial of the MET inhibitor sivotinib in patients with unresectable or metastatic PSC or other NSCLC harboring a MET exon 14 skipping mutation.
In November 2017, the patient was started on the MET inhibitor sivotinib. After 6 weeks of treatment, the first tumor assessment showed a partial response (target lesion diameter reduced from 5.6 cm at baseline to 3 cm) according to RECIST v1.1 criteria (Figure 1); moreover, the patient’s ECOG performance status score Improved from 1 point to 0. A partial response was confirmed at the second tumor assessment at week 12.
All treatment-related adverse events (AEs) reported by patients were grade 1 and included decreased white blood cell count, nausea, diarrhea, and rash. According to the Common Terminology Criteria for Adverse Events, version 4.03, AEs were grade 1 or 2. During treatment, the patient discontinued medication for 5 days due to fever (unrelated to treatment), but did not reduce the dose due to adverse events.
After 36 weeks of treatment, the patient had progressive disease (PD), and the diameter of the target lesion increased to 3.8 cm, so treatment was discontinued. After MET inhibitor treatment, the patient achieved 36 weeks of progression-free survival (PFS).
Figure 1: Imaging findings at baseline, 6 weeks (PR), and 36 weeks (PD)
MET inhibitor resistance biomarker discovery
From baseline to disease progression, the patient’s plasma circulating tumor DNA (ctDNA) samples were obtained continuously throughout the treatment period, and tumor biopsy samples were taken at disease progression. In addition, the researchers used an NGS panel of 422 cancer-related genes to explore DNA changes in tumor biopsies and plasma samples.
Analysis found that at baseline, the patient’s ctDNA showed a low level of MET exon 14 skipping mutation (c.3028+3A>G), and the VAF was 0.6%. After 6 weeks of treatment, MET-mutated VAF dropped below the limit of detection as tumor volume shrank; in subsequent cycles (18, 24, 30 weeks), and even at progression (36 weeks), none were detected. MET mutation. Except for the MET exon 14 skipping mutation, no other somatic mutations were found in the ctDNA samples.
Tumor biopsies taken at disease progression revealed the same mutation sites in the MET, TP53 and FBXW7 genes as those found before MET inhibitor treatment. In addition, NGS assays performed at disease progression revealed moderate levels of EGFR (GCN=5.7), FGFR1 (GCN=5.8), and KRAS (GCN=4.5) gene copy numbers, which were further confirmed by fluorescence in situ hybridization (Figure 2). ). This result suggests that acquired gene amplification may be associated with MET inhibitor resistance. Interestingly, NGS testing of tumor biopsy samples at the time of disease progression did not reveal MET amplification (Figure 2).
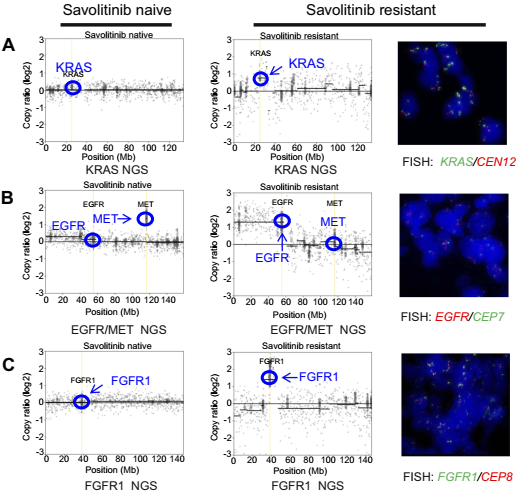
Figure 2: Copy number characterization of tumor tissue. Left column: baseline; right column: at disease progression after 36 weeks.
Case discussion
In this case, the tumor remission was rapid and durable, and the patient’s overall performance improved after treatment, demonstrating the efficacy of MET inhibitors in patients with MET exon 14 skipping mutations. Moreover, during the treatment period, patients were well tolerated with an acceptable safety profile, with no reported grade ≥3 AEs and no dose reduction required. Previous studies have found that MET inhibitors have antitumor activity against lung adenocarcinomas, including PSCs. This case provides further evidence that PSCs also respond to MET inhibitors if the MET target is effectively inhibited. This suggests that MET exon 14 skipping mutations may be a driver of NSCLC, regardless of histopathological subtype.
In this case, the MET exon 14 skipping mutation was the only somatic mutation detected in the ctDNA sample, and when a partial response was achieved, the VAF decreased significantly. The change trend of VAF was consistent with the change in tumor size, suggesting that It may serve as an indicator of tumor remission in the clinic. The absence of increased VAF in MET mutations at disease progression may be due to the development of acquired resistance that drives tumor growth (independent of MET gene status), while MET inhibitors remain efficacious MET was significantly inhibited.
Two mechanisms of drug resistance in NSCLC patients with MET exon 14 skipping mutations have been identified previously. One is target-dependent drug resistance, that is, secondary mutations in the MET kinase domain, such as D1228N and Y1230S; the other is bypass effects, such as KRAS amplification. Bypass effects were observed in this case: FGFR1, EGFR, and KRAS amplifications appeared upon disease progression. Therefore, the presence of FGFR1, EGFR, and KRAS gene amplifications during disease progression may be responsible for the resistance to MET inhibitors in this case. However, whether these genetic alterations occur in the same tumor cells or in different tumor cells, and whether FGFR1, EGFR, or MAPK pathway inhibition can restore sensitivity to MET inhibitor therapy, requires further investigation.
Interestingly, in this case, mutations in the TP53 gene were detected both before treatment and at disease progression. TP53 is the most common genetic mutation in a variety of cancers, including PSC. In general, tumors harboring TP53 mutations often exhibit a high degree of chromosomal instability, particularly mutations located in the DNA-binding domain, such as V173M in this patient. Therefore, chromosomal instability may be associated with the amplification of multiple genes, including EGFR, KRAS, and FGFR1, during MET inhibitor therapy, leading to acquired resistance. However, further research is needed to verify this association.
Summary
In this case report, a PSC patient with a MET exon 14 skipping mutation achieved clinical remission after MET inhibitor treatment, with a PFS of 36 weeks, suggesting that MET inhibitors can be effective in such patients. to clinical benefit.
References:
[1]Tong JH,Yeung SF,Chan AWH,et al.MET amplification and exon 14 splice site mutation define unique molecular subgroups of nonCsmall cell lung carcinoma with poor prognosis[J].Clinical Cancer Research,2016,22(12):3048-3056.
[2]Han S,Fang J,Lu S,Wang L,Li J,Cheng M,Ren Y,Su W.Response and acquired resistance to savolitinib in a patient with pulmonary sarcomatoid carcinoma harboring MET exon 14 skipping mutation:a case report[J].Onco Targets Ther.2019;12:7323-7328.doi:10.2147/OTT.S210365.
[3]2021 edition of “Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Non-Small Cell Lung Cancer”.
Approval number: CN-91826
This material is provided by AstraZeneca for the information of healthcare professionals only
*This information is for medical and scientific reference only, and does not constitute a recommendation or promotion of any drug or treatment plan. The information contained in this article should not be used as a substitute for medical advice from a healthcare professional.