*For medical professionals only
What should I do if I have acute renal failure with acyclovir?
Acyclovir, is widely used clinically to treat herpesvirus infections, especially herpes simplex virus (HSV) and Chickenpox-shingles virus.
However, as early as 2009, the National Medical Products Administration (NMPA) revised the acyclovir package insert, adding a boxed warning stating that acyclovir can cause acute renal failure.
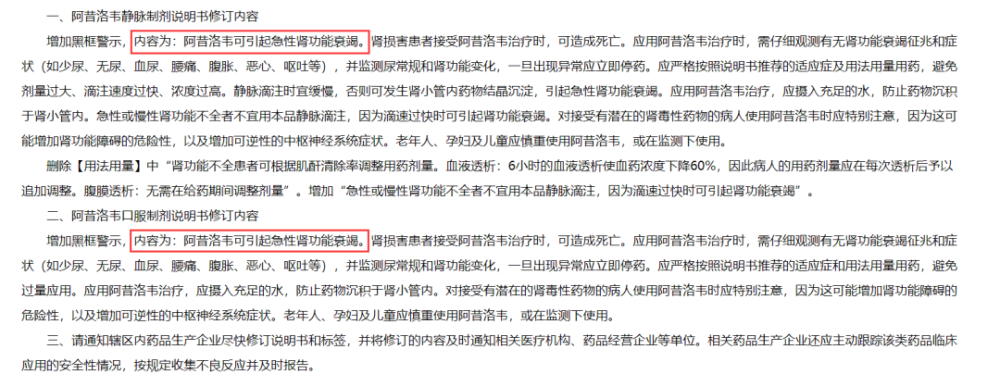
Image source: Screenshot of NMPA official website
Then, when encountering patients with acute renal insufficiency or chronic kidney disease, how to adjust the dose/treatment regimen of acyclovir, or how to assess the impact of continued acyclovir treatment risks, often confounding clinicians.
Jie Xiaoyao sorts out the mechanism by which acyclovir may cause acute kidney injury (AKI) and the feasible adjustment or alternative for readers’ reference.
01
Mechanisms of acyclovir-induced acute renal failure[1]
Acyclovir has a low protein binding rate (9%-33%), the drug is metabolized mainly through the liver, and the main metabolites produced only account for 9%-14% of the dose. And about 45%-79% of the drugs are excreted in the original form by glomerular filtration through renal tubular secretion. And acyclovir has low solubility in urine, with a maximum solubility of 2.5 mg/mL at physiological pH.
This low urine solubility and high urine output, if accompanied by a decrease in urine output, is likely to lead to the formation of crystals in the renal tubules, /strong>And with the accumulation of crystals in the renal tubules, it will eventually lead to the blockage of the renal tubules and cause kidney damage.
In addition, acyclovir may also cause direct damage to renal tubular epithelial cells, leading to degeneration and shedding of renal tubular cells, and ultimately to acute renal failure and renal tubular dysfunction.
A large number of literatures have proved that intravenous acyclovir is related to AKI, and the incidence rate is 12%-48%, most of which appear within 2-3 days of treatment, mainly with immediate onset . However, the prognosis is usually good. The fastest recovery is 2 days, the longest recovery is 2 weeks, and the recovery period is generally 7-15 days [2-4].
02
Independent risk factors for induction of AKI[2]
Renal insufficiency: Important independent risk factor for AKI (in patients with chronic kidney disease, daily monitoring of renal function is recommended for the first 2-3 days of use).
Diabetes: Important independent risk factor for AKI.
Concomitant medications: Vancomycin, non-steroidal anti-inflammatory drugs (Children should be alert to the possible AKI caused by ceftriaxone combined with acyclovir).
03
Difference between oral and IV[5-7]
Oral acyclovir has poor oral absorption, about 15%-30% is absorbed from the gastrointestinal tract. In pharmacokinetic studies, the steady-state peak plasma concentrations of acyclovir administered intravenously (5-10 mg/kg every 8 hours) were 10-20 μg/ml, whereas after multiple oral administrations (200-800 mg), this value was only 0.6-1.6 μg/ml.
Oral is mainly indicated for:
(1) Herpes simplex virus infection: It is used for the initial and recurrent cases of genital herpes virus infection, and oral administration of this product is used for prevention of recurrent cases.
(2) Herpes zoster: It is used for the treatment of herpes zoster in people with normal immune function and mild cases of people with immune deficiency.
(3) Treatment of chickenpox in immunocompromised patients.
Vins are mainly used for:
(1) Herpes simplex virus infection: used for the treatment of primary and recurrent mucocutaneous infections in immunocompromised patients and the prevention of recurrent cases, and also for the treatment of herpes simplex encephalitis.
(2) Herpes zoster: used for the treatment of severe herpes zoster in immunocompromised patients or diffuse herpes zoster in those with normal immune function.
(3) Treatment of chickenpox in immunocompromised patients.
(4) Treatment of acute retinal necrosis.
Regular oral doses may prevent therapeutic plasma levels in severe infections.
04
How to prevent and manage
Acyclovir-induced renal failure[2,6-8]
1. Fully evaluate the patient’s basic clinical conditions and medication history such as: body weight, renal function, concomitant medication, underlying diseases, history of allergies, vancomycin and non-steroidal anti-inflammatory drug use .
2. Strictly follow the instructions for the usage and dosage of acyclovir:
Dosage: The usual dose for adults, 5-10mg/kg per body weight, instilled once every 8 hours, for a total of 5-10 days, the highest daily dose for adults According to the body weight of 30mg/kg, every 8h should not exceed 20mg/kg. The usual dose for children is 250mg-500mg/m2 per body surface area or 10mg/kg per body weight, 3 times a day, every 8 hours for 5-10 days, the maximum dose for children is 500mg/8 hours per body surface area. m2.
Concentration: The preparation of the liquid in the instruction manual of acyclovir indicates that 0.5g of this product is added to 10ml of water for injection, so that the concentration is 50g/L, sufficient After shaking to form a solution, dilute it to 100ml with sodium chloride injection or 5% glucose injection, and the final drug concentration should not exceed 7g/L.
Drip speed: It is only for intravenous drip, and the time for each drip needs to be more than 1h. Intravenous infusion should be slow, otherwise drug crystal precipitation in the renal tubules may occur, causing renal damage.
Renal insufficiency: The instruction sheet states that intravenous infusion of acyclovir should not be used in patients with acute or chronic renal insufficiency, but it is not contraindicated. A study analysis found that reasonable adjustment of the dose of acyclovir did not significantly increase the incidence of AKI in patients with chronic renal insufficiency. In the absence of other alternative medicines, the dose should be adjusted for patients with chronic renal insufficiency, and careful observation should be made for signs of renal failure (such as oliguria, anuria, hematuria, low back pain, abdominal distension, nausea, vomiting, etc.), Monitor urine routine and renal glomerular filtration rate changes, and discontinue the drug immediately if any abnormality occurs.
renaldose adjustment in the event of insufficiency(intravenous):< /p>
Glomerular filtration rate (GFR): 50-80ml/min, 5-10mg/kg q8h, intravenous drip;
GFR: 10-50ml/min, 5-10mg/kg q24h, intravenous drip;
GFR: <10ml/min, 2.5-5mg/kg q24h, intravenous drip;
Hemodialysis: 2.5-5mg/(kg·d), intravenous drip after extubation;
Peritoneal dialysis: 2.5-5mg/(kg·d), intravenous drip;
Continuous arteriovenous hemofiltration: 3.5mg/(kg・d), intravenous drip;
Continuous veno-venous hemofiltration: 5-10mg/(kg·d), intravenous drip.
Dose adjustment in renal insufficiency(oral):
Table 1 Oral dose adjustment of acyclovir in patients with renal insufficiency

Concomitant medications: Avoid concomitant use of nephrotoxic medications, which may increase the risk of renal dysfunction.
Rehydration: The concentration of the drug in urine is the highest at 2 hours after intravenous infusion. At this time, the patient should be given enough water to prevent the drug from depositing in the renal tubules.
3. What to do in the event of AKI[2]
(1) Immediately discontinue the drug, and give timely symptomatic treatment including the use of loop diuretics, fluid and volume management.
(2) For patients with severe infections that cannot be discontinued, the dose may need to be adjusted, and CRRT may be required if necessary.
References:
[1]Izzedine H, Launay-Vacher V, Deray G. Antiviral drug-induced nephrotoxicity. Am J Kidney Dis. 2005;45(5):804-817.
[2] Lee EJ, Jang HN, Cho HS, et al. The incidence, risk factors, and clinical outcomes of acute kidney injury (staged using the RIFLE classification) associated with intravenous acyclovir administration .Ren Fail.2018;40(1):687-692.
[3] Wang Chunting. Analysis of acute renal failure caused by acyclovir and irrational drug use, Pharmacovigilance 2007, 4(5):268-272.
[4] Xu Bing. Clinical analysis of 13 cases of acute renal failure caused by acyclovir [J]. China Clinical Research, 2014, 27(4): 2.
[5]Lam NN, Weir MA, Yao Z, et al.Risk of acute kidney injury from oral acyclovir:a population-based study.Am J Kidney Dis.2013;61(5 ): 723-729.
[6] Instructions for Acyclovir for Injection, Standard Chinese Pharmacopoeia 2020 Edition Part II, Furen Pharmaceutical.
[7] Instructions for Acyclovir Tablets, Standard Chinese Pharmacopoeia 2020 Edition Part II, Shandong Qidu Pharmaceutical.
[8] Diagnosis and Treatment of Infectious Diseases, Second Edition.
More good articles on clinical medicine
FollowClinical Pharmacy ChannelView
Source: Clinical Pharmacy Channel
Editor in charge: Zheng Huaju
Proofreading: Zang Hengjia
Plate making: Xue Jiao