*For medical professionals only
At this year’s AAD annual meeting, the progress of AD biological therapy has become a hot topic.
The 2022 annual meeting of the American Academy of Dermatology (AAD) has come to a successful conclusion. In 4 days, dermatologists from all over the world shared and discussed in-depth the cutting-edge progress in the field of dermatology, presenting an academic feast full of dry goods.
Splendid variety, focusing on the hot topics of the conference
Atopic dermatitis (AD), as a common chronic, inflammatory and refractory skin disease, has caused a heavy burden to patients, families and society, and has always been widely accepted by the dermatology community. focus on. In this AAD annual meeting, the frontier progress in the field of AD disease is still the focus of attention.
In recent years, the advent of the biologic dupilumab has brought about a sea change in the treatment of AD. The research on dupilumab is still in full swing, and many breakthrough results have been achieved. In this AAD annual meeting, the heavy release of multiple research data of dupilumab provides a stronger basis for clinical application.
Freshly released, the field of AD disease still needs continuous exploration
AD has a high disease burden and requires long-term safe and effective control
At this year’s AAD Annual Meeting, the PEDISTAD study announced the latest research results, showing that moderate-to-severe children with AD have a multidimensional disease characterized by early AD onset, pruritus, sleep disturbance and decreased quality of life burden [1], but also has a multidimensional impact on caregiver and family life (Figure 1) [2]. This reflects the lack of safe and effective long-term treatments for moderate-to-severe pediatric AD patients [1,2]. The results of a longitudinal study, also presented at this annual meeting, show that most adults with AD, especially those with moderate-to-severe AD, have sleep disturbances; while sleep disturbances caused by AD usually improve over time, many patients experience sleep disturbances. fluctuating or persistent course of sleep disturbance [3]. Another study found that AD is related to bad behavior in childhood [4].
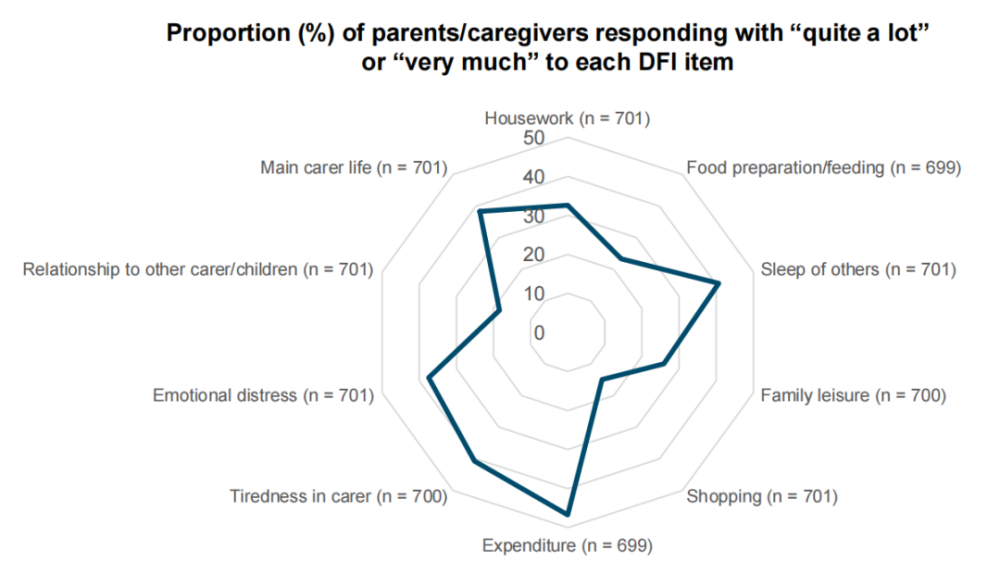
Figure 1: Family burden of children with moderate to severe AD
Traditional treatment is not enough, and the treatment plan still needs to be optimized
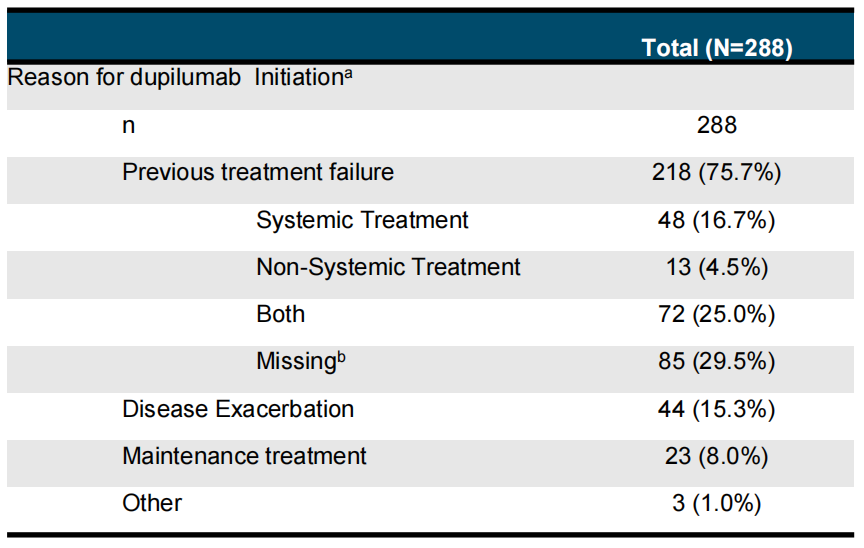
The GLOBOSTAD study presented at this AAD Annual Meeting found that up to 75.7% of adults with moderate-to-severe AD were initiated with dupilumab due to prior treatment failure (Table 1) [5] . The results of the EUROSTAD study were also presented at this AAD annual meeting, showing that 87.6%, 81.5%, and 66.3% of adult AD patients who received systemic glucocorticoids, cyclosporine, and methotrexate discontinued treatment, respectively. , the reasons for discontinuing treatment include lack of efficacy, adverse events, etc. [6]. In addition, the data from the PEDISTAD study showed that children with moderate to severe AD were basically unable to control the disease after local treatment, and immunosuppressants such as methotrexate and cyclosporine could not effectively control the pruritus of patients [7].
Table 1: Reasons for initiation of dupilumab in adults with moderate to severe AD
AD is often associated with type 2 inflammatory comorbidities, and comorbidity management strategies should also be emphasized
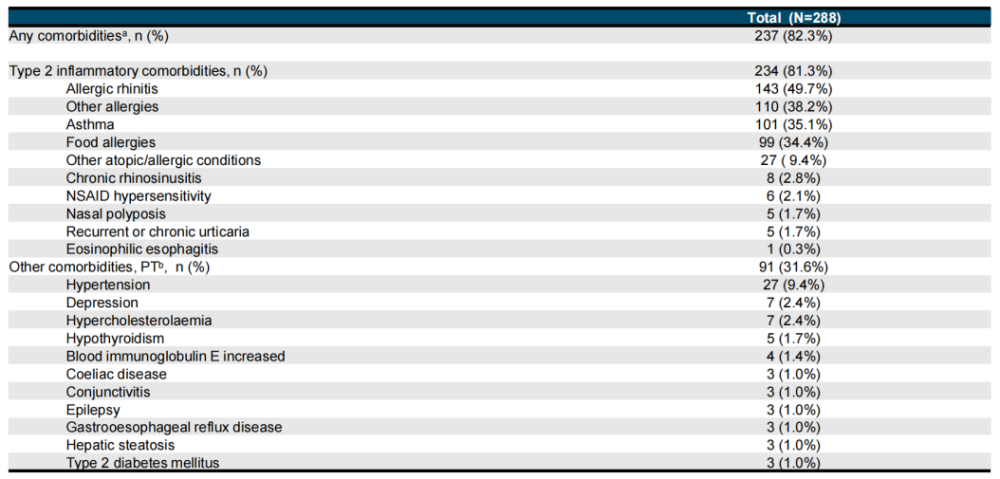
AD is a systemic disease, in addition to skin symptoms, there are other systemic manifestations. This AAD annual meeting brought a 5-year international multi-center study-GLOBOSTAD study data. The results showed that among adults with moderate to severe AD patients treated with dupilumab, comorbidities accounted for 82.7%, and comorbidities accounted for 82.7%. The proportion of patients with type 2 inflammatory comorbidities such as allergic rhinitis, asthma, and food allergy is as high as 81.3% (Table 2) [8].
Table 2: Comorbidities in adult AD patients
Heavy release, new certificate for clinical application of biologics
Facing the multiple disease burdens of AD, biologics “catch all at once”
This year’s AAD annual meeting released a number of research data on the improvement of different treatment outcomes of AD patients with dupilimumab, confirming that dupilimumab can improve skin barrier function, clinical symptoms , signs, patient-reported outcomes (PRO) and other dimensionsGood AD. For example, one study showed that 16-week treatment with dupilimumab in adolescents and adults with moderate-to-severe AD not only restored skin barrier function, but also improved various factors such as skin lesions, pruritus, disease severity, sleep, and quality of life. Dimensional implementation mitigation (Fig. 2) [9]. The results of the DUPISTAD study also confirmed that dupilumab can significantly reduce the symptoms of sleep, itching and other symptoms in adult patients with moderate to severe AD.
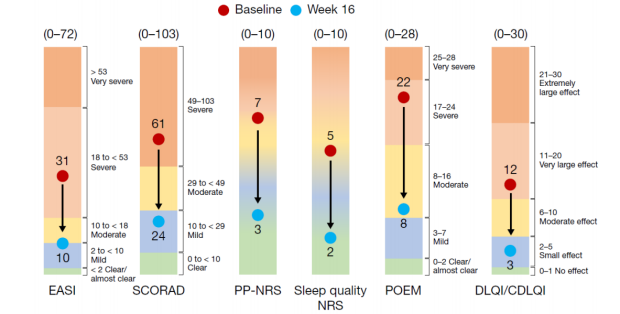
Figure 2: Symptoms, signs, and PRO improvement at 16 weeks of treatment
In addition, the RELIEVE-AD study also found that dupilumab significantly improved DLQI scores, work limitation, and mobility impairment in adult patients with moderate-to-severe AD during the first month of treatment , and can continue to improve to the 30th to 36th months [11]. It is worth mentioning that, whether in adults, adolescents, and children*, dupilimumab can rapidly improve the sleep quality of AD patients and last for 1 year [12]. These studies suggest that dupilumab can alleviate the multidimensional disease burden of AD patients and bring more clinical benefits to AD patients.
The long-term management of AD is difficult, and biologics are “rising”
With the deepening of research, the long-term clinical research data of dupilimumab have also been released, and many research results have also been displayed at this AAD annual meeting. The results of the open-label extension study (OLE) of dupilumab in the treatment of adults with moderate-to-severe AD showed that during the 4-year treatment period, dupilumab could effectively and lastingly improve the skin lesions and pruritus symptoms of patients (Figure 3) , and the safety profile is consistent with that reported in published studies of dupilumab [13]. The 30- to 36-month RELIEVE-AD study showed that early disease control can be achieved in adult patients with moderate to severe AD with dupilumab in the first month, and continued to the 30th to 36th months; At 36 months, most patients were very satisfied with the treatment [14].

Figure 3: 204 weeks of treatment, improvement of skin lesions and itching
The latest results of a Japanese study were also announced at this AAD annual meeting, which found that dupilimumab in adult AD patients can maintain skin lesions clearance and pruritus relief for at least 1 year [15]. In addition, some studies have shown that dupilimumab can maintain long-term efficacy after switching the dosing regimen from 300 mg qw* to 300 mg q2w in the treatment of adults with moderate-to-severe AD [16]. These findings reflect that dupilimumab in the treatment of AD can maintain long-term stable efficacy and good long-term safety, making it an ideal choice for long-term AD management.
*: The approved dosage for adults with moderate-to-severe AD in China is: an initial dose of 600 mg (300 mg injected twice), followed by 300 mg every two weeks. For actual use, please refer to the instruction manual of dupilumab in China, which is for academic exchange only.
Facing the real-world test, biologics help innovate AD treatment models
At present, dupilumab has been used in clinical practice for a long time. What is the actual efficacy and safety of dupilumab in the real world? What changes has dupilumab brought into the clinic for AD treatment? This year’s AAD annual meeting has successively announced the application of dupilumab in the real world. PROSE real-world evidence shows that dupilimumab treatment of moderate-to-severe AD patients aged 12 years and older for 18 months resulted in continuous improvement in skin lesions, pruritus, and quality of life (Figure 4) [17]. Dupilumab can reduce disease recurrence and improve sleep problems, skin pain, skin burning, and skin sensitivity in the first month of treatment in patients with moderate-to-severe AD. Demonstrated in the RELIEVE-AD real-world study [18].
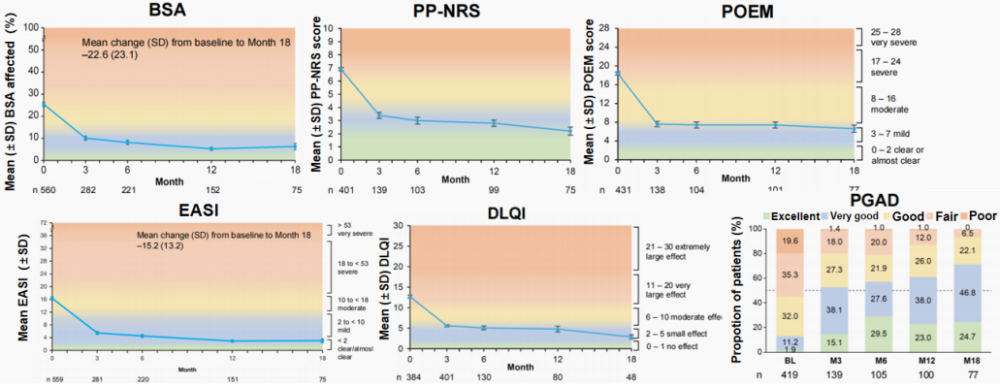
Figure 4: Improvement of symptoms, signs and PRO at 18 months of treatment
Data from another real-world study showed that the rate of skin infections in AD patients aged 12 years and older decreased from 24.7% to 11.2% after initiation of dupilumab %, and reduced the use of topical and systemic antimicrobials [19]. In addition, the RELIEVE-AD real-world study also found that the use of concomitant drugs in adult patients with moderate to severe AD was significantly reduced in the first month of dupilimumab treatment, and continued to decline during the study period; 30-36 At 12 months, up to 54.4% of patients were not using the combination [20]. The results of these studies suggest that in the real world, the treatment of AD with dupilimumab greatly improves the efficacy and safety, and simplifies the treatment plan, bringing a revolutionary change to the treatment mode of AD.
Directly targeting type 2 inflammatory pathways, biologics broaden the field of disease
Type 2 inflammatory response not only runs through the occurrence and development of AD, but is also the pathogenesis of other type 2 inflammatory diseases. IL-4 and IL-13 are the core key cytokines of type 2 inflammatory response. Dupilumab can inhibit type 2 inflammatory response by precisely targeting the IL-4 receptor α subunit while blocking the IL-4 and IL-13 signaling pathways. So, what is the efficacy of dupilumab in other type 2 inflammatory diseases? Evaluation of dupilumab therapyThe LIBERTY-CSU study of chronic spontaneous urticaria (CSU) and the LIBERTY-PN PRIME 2 study of prurigo nodularis (PN) have been carried out, and the latest research results were announced at this AAD conference.
LIBERTY-CSU study results show that 24 weeks of omalizumab-naïve omalizumab-naïve patients with moderate-to-severe CSU can significantly improve itching, severe urticaria, and pruritus. and urticaria activity (Fig. 5), with acceptable tolerability and safety [21]. The LIBERTY-PN PRIME 2 study showed that 12-week treatment with dupilumab can significantly improve pruritus response and skin lesions in adult PN patients, and the safety is consistent with that of dupilumab [22]. The publication of the results of these two studies not only confirmed the good efficacy and safety of dupilumab in the treatment of CSU and PN, but also suggested that dupilumab has potential efficacy in other type 2 inflammatory diseases. We look forward to more research data in the future to provide evidence-based evidence for the application of dupilumab to other type 2 inflammatory diseases such as CSU and PN.
*: Dupilumab has not yet been approved for CSU and PN indications, and this is for academic exchange only.
Figure 5: Improvement in pruritus, urticaria severity, and urticaria activity at 24 weeks of treatment
Summary
In summary, the treatment of AD has always been challenging and requires constant exploration. The good news is that the advent of dupilumab has rewritten the treatment pattern of AD to a certain extent. At present, dupilumab has accumulated rich evidence-based medical evidence and clinical practice experience, and will continue to conduct more in-depth and diversified explorations in the future to better benefit the majority of patients with skin diseases.
*: Dupilumab is currently only approved in China for moderate-to-severe AD indications in children and adults aged 6 years and above who are poorly controlled or not recommended for topical use.
References:
[1]Amy S. Paller, et al. AAD 2022. #P33548.
[2]Marjolein de Bruin-Weller, et al. AAD 2022. #P34021.
[3] Jaya Manjunath, BS, et al. AAD 2022. #P32703.
[4] Jaya Manjunath, BS, et al. AAD 2022. #P32702.
[5]Silvia M. Ferrucci, et al. AAD 2022. #P34332.
[6]Marjolein de Bruin-Weller, et al. AAD 2022. #P34574.
[7]Eulalia Baselga, et al. AAD 2022. #P33553.
[8]Piergiacomo Calzavara-Pinton, et al. AAD 2022. #P34329.
[9]Robert Bissonnette, et al. AAD 2022. #P33557.
[10]Joseph F. Merola, et al. AAD 2022. #P33558.
[11]Dimittri Delevry, et al. AAD 2022. #P33325.
[12]Amy S. Paller, et al. AAD 2022. #P34297.
[13]Jacob P. Thyssen, et al. AAD 2022. #P34358.
[14]Bruce Strober, et al. AAD 2022. #P33120.
[15]Hiroyuki Fujita, et al. AAD 2022. #P32501.
[16]Lisa A. Beck, et al. AAD 2022. #P34385.
[17]Jerry Bagel, et al. AAD 2022. #P34313.
[18]Bruce Strober, et al. AAD 2022. #P33322.
[19]Peck Ong, et al. AAD 2022. #P34326.
[20]Dimittri Delevry, et al. AAD 2022. #P32929.
[21]Marcus Maurer, et al. AAD 2022. #P33004.
[22]Gil Yosipovitch, et al. Presented at 2022 AAD. Boston, MA, USA; March 25-29.
Approval number: MAT-CN-2205144 Valid until: December 31, 2022
This number is only used as Sanofi’s confirmation of the authenticity of the scientific and clinical data sources in the therapeutic field of Sanofi-related drugs involved in this article, and does not serve as Sanofi’s accuracy of the entire content of this article Confirmation and assurance of validity, timeliness and completeness;
This article is for use by healthcare professionals for academic communication or medical information purposes only, and does not constitute a recommendation or promotion of any drug or treatment. The information contained in this article should not be used as a substitute for medical advice from a healthcare professional. This information is for medical and scientific purposes only and Sanofi does not recommend the use of this product in any manner inconsistent with the prescribing information approved in your country. This material is intended for use by healthcare professionals only.
*This article is for the purpose of providing scientific information to healthcare professionals only and does not represent the platform’s position